Cards on the table: I like to write. Maybe a little too much.
It’s inconvenient to have crapped-out wrists that limit typing severely and a voice just weird enough in accent & vocal fry to make dictation software stare back at me, blinking blankly, instead of capturing the marvelous flow of inspiration…
Yeah. To heck with that. I have to make it simpler.
I have a bunch of self-documentation templates and techniques which I’ve been meaning to write about, because we know how important providing evidence of your own experience can be and because… I like to write.
Sigh.
I’m not trying to make them pretty and I’m certainly not taking the time to make them generic or pare out the details of what I’ve tried and used over the years. I like doing that, but wanting to do that is what has kept from getting this stuff up… for years.
I’m just going to throw them at you instead. You’re all smart enough to take what you like and leave the rest. Have fun!
Note: All of my Self-Documentation by LivingAnyway.com is marked CC0 1.0. To view a copy of this mark, visit https://creativecommons.org/publicdomain/zero/1.0/
TL;DR – it’s a formal way of making this work Public Domain. Go wild. It’s yours now.
Pro Tip: There are good health tracker apps now, and one or two are very good. If they work for you, that’s good enough!
If, like me, screens hurt your eyes and tapping hurts your hands, you might want to consider the ol’ pen-and-paper method here.
We’ve got logs in color. We’ve got ’em in black and white. We’ve got half sheets, whole sheets. We’ve got tables, checkboxes, body maps… anything I could think of to make using these a low-cognition task:
You can see how my tracking changed depending on just how sick I was vs. how much activity I could (or, more often, wanted to) expect from myself. They show how my priorities and needs shifted, what worked for me well enough to track, and so on. Don’t worry that it seems rather personal – it’s all information; information is a good thing; good things should be shared. You might find a relevant format to start your own tracker from.
They’re in PDF format, for technical reasons. Conversion tools and PDF editing tools are available, some of them for free. Have fun, and come back here to re-download if you mess something up. This is a no-shame zone.
Having crashed and burned in a (for me) spectacular manner, I’m being (ahem) encouraged by many of my nearest and dearest to stop pretending I’m so much healthier and stronger and more multi-systemically resilient than I am.
My underlying state of health is not good, and I hate discussing it. It’s tiresome and depressing. That said, ignoring it obviously doesn’t work for long. Need a 3rd way.
I’m pushing 60. Time to stop pretending I’m 34… which was my last year of what I still reflexively consider my normal health & athleticism, and it was also when this pain syndrome was laying down its first tracks. Between multiple bereavements, recurring respiratory infections, and repeated courses of megadeath antibiotics, my nervous system was primed for disruption.
As one friend said, “We habitually present a version of our pre-CRPS selves” and, outside my 4 walls and the privacy within, I don’t seem to have anyone else to be yet. How can I exist without coming off as hardy and buoyant? I don’t know what that could even look like.
I go out and do things in public view, then crawl home (nope still no car, yes it’s been all of 2025, yes I’m struggling more all the time, don’t ask) to recover in private. Those are my 2 gears. I’ve recently developed a half-gear of being in my garden plot, but that now requires a lift because the bus is too brutal – although I love that it’s currently free!
It feels like I’m waiting for the world to allow me to heal. If that sounds self-pitying, you’re probably right. I’m new to un-masking, and it’ll take practice to get the tone right – un-self-pitying, but fully honest for a change.
Showing showering
I’ve been drawing cartoons of lives like mine for years. I was waiting to put them into a book, but they’re doing no good in my folio and some have been there for way too long. I’ve also drawn communication tools. It didn’t seem time to share them before, but it sure does now.
First up…
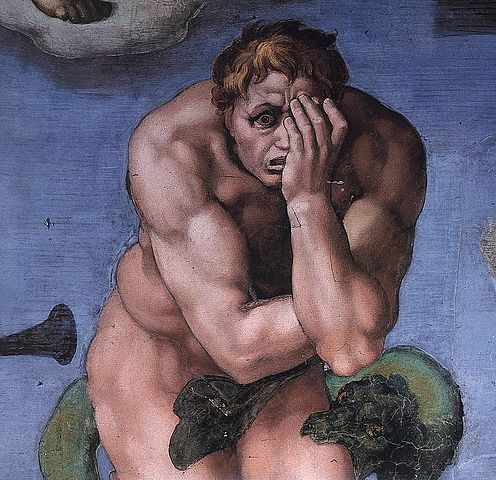
Taking a shower on a bad day:
When I’m rash enough to shower on a bad day, it feels kinda like this.
This picture isn’t finished, but it’s good enough. You can enlarge it to see the way the (to my senses) appalling changes of temperature wrap around every individual drop’s path all the way into the drain.
I couldn’t find a way to draw the way each drop feels like there’s a hook in its head, physically latching onto and dragging energy out of my body. That doesn’t hurt (unlike the hot/cold nonsense) but boy, is it exhausting!
So, when you can tell (pew!) that I haven’t had a proper shower or even gotten wet recently, you’ll be able to surmise that the pain has been higher than my ability to cope with the intensity of the experience.
For the record – I gritted my teeth and showered & washed my hair yesterday morning! I’m taking a bow, frankly. I had a familiar audiobook to listen to, which sometimes can keep my attention off those hot/cold and dragging sensations.
Keep in mind that everyone’s pain is their own. CRPSers don’t all have the same experience in the shower, because, for some, it’s awful in some other way. Not all days are this bad, even 24 years in. Nuance is key. Also, boundaries.
My pain isn’t yours, and nor should it be.
The idea here is to give you a chance to look on, without looking for anything more than your witness. That right there is a powerful thing: just being seen.
Don’t take it on. Just adjust your expectations, maybe, as I’m learning to do myself.
If you’re a bio-nerd, read up on how humans go from mad mitosis to having skin and organs. It is absolutely fascinating – and explains a lot about neurological variations!
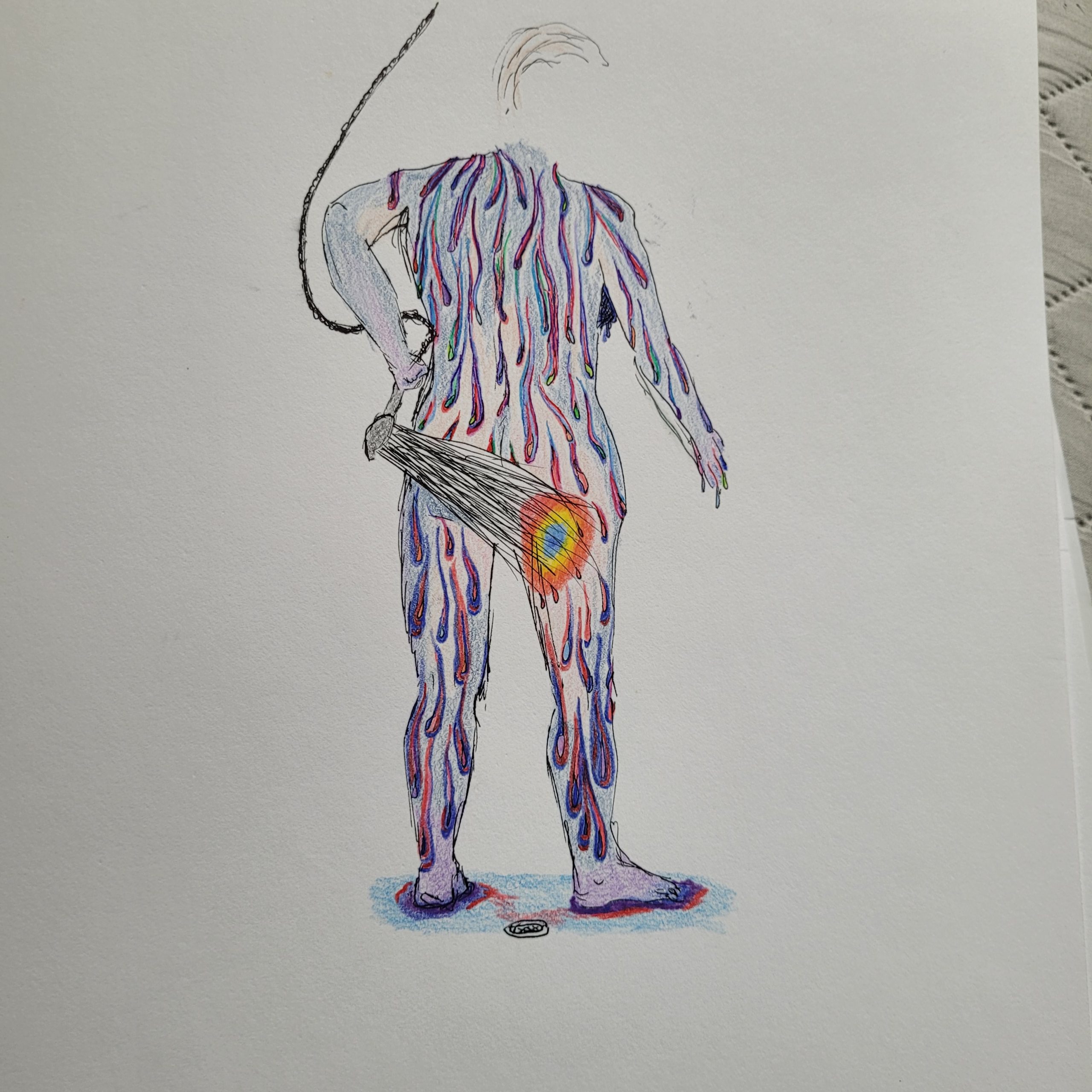
Communication tool: moods & self-care
I’ve also got a delightful communication tool to share.
As we all now know, my mood may not reflect the outward, apparent situation. There can be stuff burbling away that affects me in ways I might not realize, but others can.
I came up with a rough drawing of a rating scale for my housemates to use (when I had some) and it was a huge help to get that objective feedback – without anyone being defensive! I’d sometimes find the magnet moved to a different number, then go away and take care of myself until I was pretty sure it could move back up. Usually, though, they felt free to call me over and show me where my behavior was, and I loved their honesty. Did me a lot of good.
I particularly like how it indicates when a level of irritation is appropriate. That was a mind- blower for me, as I’d been telling myself that it was always bad to be unpleasant. Nope! Sometimes it’s perfectly appropriate!
I think, and hope, that sharing these images and tools will:
A. Be useful, and
B. Get it right through the concrete (taps own head) that I need to come up with ways to live and engage with the world that are congruent with this reality.
My inner Cleopatra, queen of de Nile, needs to get back to Egypt.
Cheers and virtual hugs are most welcome! I’m daunted by this job. I mean… I value honesty enormously… just not about my weaknesses and disabilities 🤣
This is a long one. Grab something to drink and put your feet up, if you want to…
In the wildly unlikely event that, say, a vulnerable American citizen felt moved to respect the anti-immigration feeling and return to the lands that, say, my ancestors left in the 1600s and 1700s… how would that work?
It helps if you already have a passport. This is important. Go here:
and follow the instructions there – whenever you land on it. Passports are issued by the State Department, and the State Department is currently being defunded and depopulated, so their processes may change.
This hypothetical traveler – let’s call her Max Peregrine – and why not? – is female, disabled, poor, and has very short hair. This puts her in several categories of risk in the US in 2025, and she’d like to know what other options there are for someone like her. Her service animal, a minature goldendoodle, has to go with her.
This is important.
Max has learned that a pet leaving the US has to get a certificate from a vet specifically qualified to issue international pet health certificates. She asked her usual vet, who referred her to the USDA web site to find one.
The USDA has been running increasingly lean for years, and has recently been gutted by the incoming president and his team, so the list of vets qualified to give this pet health certificate is out of date.
Max has been disabled a long time and is used to this kind of disappointment, so, after an Epsom salt bath and a TV break, she called down the list of veterinarians in the area until she found one who can (theoretically) give this certificate.
It took the one vet she found 3 weeks to research whether this is even possible. The USDA (which supervises animal health certificates for travel) is running out of staff, after all, and every country people want to bring their animals to has its own peculiarities over what is required to clear a pet for arrival, so it gets very complicated very quickly.
Sadly, the information that non-vets like Max find about import requirements is less than half the story.
Also, the US export process is complex in itself, and requires a 3-hour minimum turnaround between the vet and the USDA for the form to be submitted, reviewed, inspected, corrected, approved, and printed out. That is, if nothing goes wrong.
This vet certificate has to be issued within 10 days of departure (in some cases, 3 days, depending on the country the traveler is going to) so it’s good to start this process well in advance, and be willing to stay flexible.
If, like Max, your pet had an uncertain history or belongs to someone with limited mobility, it’s possible you’ll hit a snag: if the initial rabies series was not done exactly right, you might have to start the series over, do a blood test in 3 weeks, and be sure to get the next one inside of a year.
If you travel to Europe, you’re in luck: go to a certified vet there and get your pet an EU Pet Passport. It’ll make everything a lot easier as it’s widely accepted.
It’s important to remember that Max belongs to a category of people who can’t afford a package trip, nor a concierge trip. She has to do all the planning and reservations herself, and track all that info if, for instance, her pet’s initial rabies vaccination did not happen exactly as intended, and every leg of her trip has to be adjusted, by herself, one piece at a time.
Every transport company has their own pet policies, so she also has to call every single carrier in the chain of the journey to make sure her pet reservation has followed her.
It’s fortunate for Max that her executive function happens to have extra bandwidth for travel planning. It’s in her DNA. Her ancestors have been traveling for at least 350 years.
Since Max’s mini goldendoodle, a girl named Sam, is a Service Animal, there’s no question of that pet being refused. She has to fly with her person.
However, her paperwork still has to be in order!
So, having rectified the rabies shot situation, changed the entire trip to 2 weeks later to make sure her dog can come, and found half a dozen places to get food that matched her dietary requirements in each place she planned to stay in, Max was smart enough to know she could not possibly relax until she actually had her toes in the sand and her dog in her arms at the same time. The preparation for this trip had only just started.
Max is probably a bit overwhelmed, but can get good advice and good tools. She got Smart Tags for her luggage, found friends willing to be phone buddies to use Find My Phone to watch her progress, set an alarm to remind her to turn on Location and 5G at every transfer to give Find My Phone a signal, and then returns to low-rad mode so she’s not battling cyclical vomiting syndrome (which is what happens when she’s around too much signal too close to her body) while conducting a long trirp.
Cyclical vomiting is never fun, but it’s worse all around when you’re packed into Economy class.
Max, who hates travel surprises and likes to be organized, has also prepared a travel folder with pockets and tabs:
Complete itinerary in the inside pocket in front.
First tab: Check in information for each stage of the trip. This also proves that she plans to return in less than 90 days, because that’s important in an increasingly immigrant-hostile world.
2nd tab: Visa related info: trip insurance coverage, with the coverages page copied and stapled to the front for easy reference.
3rd tab, more visa related info: Lodging reservations, printed in every language she’ll be travelling through, so each border can conduct its own checks. Arriving with nowhere to stay is a big no-no these days; no more turning up and finding the nearest hostel.
Health tab: vaccination info. A lot of places really care about this, so get your shots if you want to travel, and get printouts from your provider. If you can afford it, you can have a travel specialist doctor make a yellow International Certificate of Vaccination, which is accepted everywhere – like the best credit cards.
Emergency: this tab is particular because Max has underlying medical conditions. There’s a MOLST form, which providees instructions for when someone is unconscious and can’t tell you if they want CPR or oxygen. It should also have copies of prescriptions, which you can get by calling your pharmacist and asking them to print them out. (Some countries require prescriptions hand-signed from the doctor’s office, but electronics are making their way into this process more over time.)
The pet, naturally, has her own tab. Her health certification, rabies documentation, and whatever else is needed, go here. This includes her microchip number, because pets require a chip for travel.
At the back of the folder, Max has left space to keep brochures and flyers for things she most wants – from safe places to get food, to inexpensive trips, free/cheap sights, and bus schedules. Max looks forward to filling that up, but knows she has to be careful with money because she’s still poor … she’s just staying somewhere a lot cheaper than her home at the moment, somewhere the government is not (yet) committing very messy self-merc.
And then there’s packing. Max has to bring her own self-care mechanisms, which involve a lot of pillows and some extra gear. Being disabled is a lot of work and there’s just no getting around that. Everything that’s most necessary for that work has to come with, or be bought there, and she’s on a tight budget.
Happily, sunshine is free!
Max is an expert at enjoying the little beauties and making the most of whatever blessings come her way. She’s going to have a fabulous time, and so is her service animal.
I’m a little envious, but I’ll be sticking around for the foreseeable. I helped Max with some of her research, though, so there’s likely to be more to come…
This article is utilitarian. It provides descriptive terms for people with similar experiences to use in communicating with their doctors, payors, and loved ones.
It discusses the impact of an ordinary household task, and explains why doing such an ordinary thing could, in fact, be unthinkably difficult for people with certain neurological issues, even though their arms appear to function reasonably well.
It aims to mitigate some of the effects of the invisibleness of pain- and sensory-related disability.
Washing dishes is a problem. It’s never been fun, but it has been satisfying, because, talk about instant gratification: you do something and things are immediately better! I liked that!
Hoping for more autonomy, I recently got a great pair of washing-up gloves. Here’s what I’ve learned.
The problems with washing dishes are:
– The way water over the hands, which are rich in nerves, intensifies sensation and creates constant tactile input that multiplies every other sensation. I think it also has an effect on electrical conductivity in my hands and, as we know, the electrical conductivity in my hands is a complete mess anyway. This is where my CRPS started.
– Hot and cold temperature variation. This activates the C-fibres in my hands and forearms, the nerves that transmit hot and cold and itch and pain. My body has trouble distinguishing between those sensations. So as the water changes temperature – down to fractions of a degree, which most people would not even be aware of – my nerves and the blood vessel activity that the nerves can command are all just having a little meltdown.
– Because of histamine issues and allergies , most of my dishes are glass or metal. Both of those substances have a strong impact on my tactile sensation. (They’re hard to touch and uncomfortable to use, but I have to use them.) I think this has something to do with how extravagantly they conduct temp and, in the case of metal, electricity. Both of which translate to discomfort and pain and impair my ability to control the motion of my hands. This muscular impairment is a characteristic of long-standing CRPS.
So, between having to juggle all that sensation, all that pain, all that vascular/tactile disruption, and the loss of muscle control that comes with it, washing dishes is a real problem for me (cf. taking a shower. Another post for another day.)
Think about dropping glass and fumbling knives, and you’ll see what this means in practical terms.
My cat has learned how to respond when I break glass. She comes to the edge of the splatter zone and meeps to check in on me, then sits out of the way but in sight, supervising the entire process from picking up big pieces to sweeping the rest and finally getting up the tiny shards with large damp rags. Only then does she enter the zone and check my work! She doesn’t let me forget how important it is to clean it up properly, and comforts me considerably during the subsequent recovery time.
I got some dishwashing gloves, hoping they would help. What I’ve found is:
– They eliminate the water contact – until my hands start to sweat. Since they are necessarily an artificial substance, this happens pretty quickly because that’s how my skin responds to manufactured surfaces. The term for this is “sudomotor reflex.”
– They reduce the temperature variations, but not as much as you’d think. I’m astonished, myself, to find just how sensitive these hands are to tiny temperature changes. This relates to “thermoregulation” and “thermosensation” problems in CRPS.
– They do help somewhat with dexterity because they’re nice and grippy. However, they don’t fit well because they’re a generic size. With the quick sweating and the temperature changes, the dexterity problem really isn’t resolved.
– I don’t have to come into direct contact with the glass or metal, and that does mitigate some of these issues. It’s just that they’re not the only issues.
The peculiar nature of peripheral neuropathy with CRPS makes this pretty much unwinnable.
So I guess I still need someone else to do my dishes.
If anyone can think of a way to rinse and load a dishwasher and then remove the dishes when they’re clean and dry but still solves the problems of water, dexterity, glass and metal … I would be happy to hear it.
I’m posting this not to whine, but because it can be so very hard to articulate these profoundly abnormal sensory experiences, and I know I’m not the only one to have them. As always, please feel free to link and copy, and I’d prefer it if you point to this webpage if you put this in print or online. Thank you so much! In the end, if you need to use it, then just use it. Spoonies unite.
Speaking of spoonies uniting…
The fact that this post got written without me going into a complete fugue state and wandering into traffic, or somewhere equally unlikely, is thanks to Elle and the Auto Gnome, who kindly took dictation — and kept me from wandering off in an effort to avoid thinking about this any longer than necessary! It’s a ghastly situation and my usual coping method is to articulate a ghastly situation once, and then focus on workarounds, spending as little further attention as possible on the ghastly thing itself.
I saw a whole lot of stars last night. Good for the soul, that.
I’ve been taking this opportunity to be in the experience of life without having to explain it, or articulate reasons to anyone outside my own skin. I had almost forgotten what that’s like. With very bright and articulate people in my life, it’s hard to get that in my personal life. Their need to understand is borne of pure love — they worry, because they’ve seen me through some rough times, and in order not to worry too much, they need to understand in their own minds what’s going on in this mind over here, which is in a completely different person. (Mom, you’re in good company with my lot! <3)
I’m in a lot of “thin end of the bell curve” categories, so this can take some doing: INFP (about 2-4% of the population, last I heard), serendipitously rather than linearly accomplishing (about 20%), and ADHD female (goodness knows, but the proportion seems to be growing as the markers are better understood), in addition to the weird requirements of all these illnesses — pretty much guarantee that anything normal won’t work, no matter how carefully I plan and execute.
This is the second summer in a row where things have not gone according to plan, so much so that a new term somewhere between “not according to plan” and “WTF just happened” needs to be coined to express it. I’m beginning to think I should just take this as a new life pattern, since the switchbacks tend to heal the dribbling wounds of layers & layers of PTSD. (Well-managed PTSD is not the same as resolved PTSD, although the most dramatic difference is on the inside.)
My friend and honorary BIL Ron wound up with massively metastatic liver cancer because 2 years of pandemic disruption and lousy treatment from LA’s indigent support system (which is a criminally bad system, worse than war-escaping migrant camps and most internment camps, according to the UN) left his early, localized, treatable cancer as an undiagnosed blurch on a CT scan which he had a few months before the pandemic was identified.
His care was denied because there weren’t enough staff or open beds. He was killed because of, but not from, Covid. When you think about maskless people and Covid deniers, think about treatable, localized cancer turning into a deadly and agonizing bloodbath for people like Ronnie.
Yeah… I’m not bitter… much!
Folks, this is not a drill. It’s not imaginary. It’s a fast-evolving pandemic in its early days. Read up on the Black Death for a little perspective.
A couple months ago, as people told themselves the pandemic was “settling down” right before the peak of record-setting waves of contagion and death (check the data, not the ideology) Ronnie bent down to pick something up, passed out, and woke up in hospital getting the third of eight units of blood. Then he found out over half his liver was lost to cancer and that treatment would only buy him a matter of months.
He opted to skip treatment and make the best of his remaining time.
He wanted to go fishing, so he set his mind to get strong enough for one last boat trip. His family proposed bringing him home to Northern California, where there’s glorious fishing in all sorts of waters.
Long story short, the appalling facility he was in was so good at losing contact information, that his hospice social worker didn’t realize he even had family until I had the option of including a gift card with a care package I sent from Amazon, and I included four names and numbers. Then things started happening.
If you’ve got someone in a facility, send them a card! It’s documentation that people care, and nothing happens in health care without documentation!
I never thought of it as anything other than a nice gesture, but turns out it’s a whole lot more: It’s evidence that they’re worth saving. ÷O
Put your number on it if they’re in bad shape, so the facility has someone to call. Atrocious that this should be needful, but hey, welcome to modern America! o_O
OK… maybe a *little* bitter.
Since I was about ready to have him kidnapped to get out of that stupid facility, we had contingency plans up the wazoo to get him out of there and home.
Even longer story short, it turned out that the only feasible option was to drive him home, which was a 2 person job and only one person in that elderly and health-challenged family could do that, so I changed my own plans (plan is a 4-letter word anyway) and got the soonest ticket I could.
As he listened to this planning conversation, Ronnie smiled from ear to ear with tears streaming down his face. He could take in how much he was loved and wanted, and he was going home to a slice of paradise to be surrounded and supported by the care of those who loved him.
Important note here: he already had this information, but he also had his own layers of damage which made it hard to let the information in. That resistance was there for a reason. You can say something to someone all you want, but if they aren’t equipped to accept it, it won’t go much further. There has to be a big enough change in themselves and their circumstances for those scars to shift, so the info can flow.
Ron was able to put aside everything that kept him from being able to accept that information, and he had, as the wise social worker said, “a moment of pure happiness.”
The following day, his condition deteriorated. We updated our plans to go visit and hope for the best.
The morning I was supposed to fly out, he was gone.
I did my quiet-inner-voice thing, and it said “go anyway.” So I did.
Bodhisattva oath
I’ve been contemplating the distinction between working the Bodhisattva vow and being a doormat (or codependent, as we call it now), off and on, ever since I discovered the concept when I was 12 or 13. It’s been an important part of my work of dealing with the last couple decades of harrowing illness, poverty, and systematized abuse as a patient. It’s become a regular topic recently in my meditation class. This is a big deal and an important point to consider.
The difference, it seems, is about self-care and responsible boundaries. These are particularly key for people who are women, healers, and in a vulnerable situation; it may not have escaped your notice that the wording which defines these terms was developed by men who had quite a bit of support in their work, and such people need a lot less protecting.
It’s healthful for people in habitual authority/access/power over others to embrace a practice of profound and selfless compassion. It gives them more insight and calm.
Those of us whose ground state is based on acute awareness of others require a more nuanced approach.
There are techniques which allow a diligent practitioner to pursue the Bodhisattva vow over the rim of what appears as boundaried behavior without psychological damage, but they only come after many years of serious training and discipline with qualified supervision. So, people like me have to be pretty darned careful how we proceed.
In short, I was in two minds about my own reasons for coming, but I yielded to the quiet tidal bore of my inner voice and took that flight.
Serendipity
I’ve landed in a beautifully imperfect place among people who wear their glorious sweetness and relentless flaws in flowing symmetry. From Ronnie’s kin, I’d expect nothing less.
Above all, I realize it’s not my bathtub to soak in and not a set of problems for me to fix. I’m just here as a welcomed guest and loved part of this extended & protracted family system.
This is a big deal.
There’s a lot of work for me to do (administrative nonsense, since death and life are both business matters; my trip will be paid for) and that’s healthy, because it’s easy for me and a real boon to the family. Healthy boundary there.
There is a lot of soft, verdant ground for me to walk on; a ton of stars spilling across the sky overhead; a cornucopia of Isy-friendly food pouring out of the greenery on this well-kept land; and my allergies have backed off considerably. My ex has put my health needs absolutely first in every consideration and the rest of the family is happy to support that. Definitely healthy.
And me? I’m not over-explaining! It’s amazing :D! I just quietly take care of my needs and appreciate everything that I *can* partake of. Good boundaries there, too.
I’m learning, carefully, again, how to be present. How to unlock from anxiety without letting go of my real needs. My phone is nearby and in signal, but usually off. That’s healthy too, right now. It’s a kind of technology break, which my battered and hyperactive brain is probably long overdue for.
I’m also bereaved in the presence of others who are also old hands at bereavement. It’s a peaceful thing. It feels curiously wholesome, even as grief and mortality are shredding sorts of events. Ronnie and all our late loved ones are very present in their very absence.
I could natter on about the wheel of life and possibly even spout some Buddhist wisdom about interconnectedness and emptiness, but to put it in words is to miss the point. It’s an experience. All you can really do with an experience is to be in it and allow it to be part of you.
So that’s what I’m doing. And there’s real healing in it.
For some things, no explanation is needed because, at root, none is… oh I don’t know… possible?
Anyway, I’m OK. I’m doing the things and being the me and accepting the limits (including transport) while appreciating the strengths (like interconnectedness) and feeling very secure and centered and remarkably peaceful withal. This is good. And if my phone is off, be assured it would be on if I needed it. Right now, the stars and the green and the peace are healing me, and I’m simply letting them. <3
Over the past 14 months I’ve gotten a look at every house I found that was:
1. Already built,
2. In my price range & size range (600-900 sq ft),
3. Judging from the ad, might qualify for a first-time homebuyer loan (which I could get, because sailboats don’t count as homes in this context. Considering how much work sailboats are to live on, I think that’s just precious.)
All 4 of them.
In 14 months of sporadic, but persistent, looking… only 4 houses turned up within my parameters.
Well, actually, only 3 were in my parameters. It just looked SO pathetic, I threw in the house I looked at that taught me just how horrific it could be to buy a repo. I don’t know why I felt a need to count that.
So, really, 3 houses. Only 3 even seemed possible, but they weren’t. They turned out to be marginally too fuddup for the loan, too moldy, or too close to too many Isy-toxic things.
Broke my heart.
The Market
In all this time, there were 2 houses I wanted to view that did, in fact, meet all 3 criteria, but they had a buyer and 5 alternates before I even had a chance to reach for the phone. Good, small homes go FAST here! (If anybody’s looking for steady returns on moderate investments, consider building some, eh? I’d be happy to project-manage that business. It’d be a great example of doing well while doing good.)
Double the target size and price point, and I’d have LOADS of options. The market is littered with 1200-2000 sq ft pocket palaces for a quarter to a third of a mil. Those buyers can be as fussy as they please around here.
The Reality Check
Here are some grim financial realities which bring new depth to the yawning chasm of the imp-possibility of me finding a safe home:
1. Frail, reactive body on SSDI.
NOTE: It’s illegal for anyone on SSDI (which normally brings in government-sponsored health care) to have over $2,000 in personal assests (exempting already-owned house and car), ever at all, even for 1 day, or they can stop your health coverage.
You read that right, folks. In the USA, poor and sick/disabled people are brutally barred from saving up, even in the interests of getting a car or home if they don’t already own one. (That was a GOP mandate. How’s that for fiscally responsible? /headdesk/)
2. Only legally-recognized close relatives are allowed to contribute to a mortgage. No matter how well connected the PDSP (Poor Disabled Sick Person; or, if you’re from California, Person who’s Disabled, Sick, and Poor), or how wide and generous their circle of friends, *nobody else* is allowed to contribute, or else the PDSP *gets no loan.*
NOTE: this was nominally an anti-terrorist maneuver, to keep cells from easily acquiring property. Which makes even less sense than most modern American anti-terrorist legislation… ‘cuz somehow the financial data-mining that’s actually been built into your central processing chip since the turn of the millenium, and is now supplemented by every data stream you dip into, is magically unable to track the source of these gifts, in this one realm of financial transactions? Huh?? And somehow it assumes that terrorists can’t find other ways to meet their logistical needs — a counter-factual assumption, at best. I grew up with actual terrorist threats framing our daily lives; this mickey-mouse magical thinking irritates me at the best of times.)
3. First time homebuyers (c.f. the snarkery in the opening paragraphs) get automatically lined up for a loan called FHA, which banks appreciate because the loan is insured by the feds. All houses bought with that kind of loan have to meet certain standards before purchase.
NOTE: this is generally good, as it ensures that first-time homebuyers start out in a code-compliant home. For me, it’s disastrous, because the standards don’t account for occult mold or proximity to fossil fuel output and EM radiation — but they heavily favor fresh paint and conventional insulation, cheap and reasonable ways to meet the code criteria. These amount to life-or-death issues for me.
4. Ordinarily, it’s extremely difficult — in fact, well-nigh impossible — to get a “one mortgage” or build loan, which you can use to buy a lot and have your own home built on it. Too many people have taken the money and run, or gotten overwhelmed by loads of decisions and delays they’re not used to, or lost their way somehow. This leaves unfinished properties dissolving where they stand, and frustrated loan officers doing much the same thing.
Now, when those loans ARE made, payouts are structured to keep the owner one large payout behind. The idea is to make sure the owner has “enough skin in the game”, a metaphor I always hear in this connection, which is peculiarly apt and especially painful for someone with CRPS.
Also, you need a builder on board who is prepared to advocate with the bank. How many builders really want to face a freaking bank just to get a picayune, weird little job like mine?
Also, my builder would have to be someone comfortable enough with low-tox building to help me be rightly understood when I talk about using high-grade materials in what’s otherwise a cheapest-possible design.
The Current Scenario
So, here’s what I bring to the table:
1. Frail, reactive body needing a small home with nonstandard finishes. Have some resources and loads of information.
2. Some relatives are able and willing to contribute, thank heavens and them!
3. Friendly mortgage broker, glad to work with me and guide me in inserting my info into their system in the most fruitful possible way. (Applied Mortgage in Northampton, MA. I recommend them very highly!)
4. Doctors willing to provide letters on letterhead stating that I do, in fact, have demonstrated needs that affect my safest home environment, and it would be good to work with me on that. (If only their fax machines worked.)
5. Info and analysis by the bucketload, which only needs to be extracted from my brain and the web and dumped out into tables, spreadsheets, breakdowns, overviews, digests, summaries, etc., about just what’s needed and just why it matters and what it really does to me when it doesn’t happen right. With references and bibiliographies for key concepts and key resources. In colors and patterns that are meaningfully coded to the info. In as many copies as they like. In origami folds, if that would help. Tied up in a neat little ribbon — green, as a hint. Sound good?
Of course, given 3 functional hours each day, putting that together is so much easier than it sounds… NOT. If I don’t go out and run errands or appointments, or eat anything the least bit wrong, get only a short walk in as exercise, my voice recognition software has no trouble with my allergy-hoarse voice, and I take 20 minute breaks every 30 minutes absolutely faithfully, I can try to eke that out to as much as 5 productive hours per day!
Who knows, it might happen!
Sysiphus was an amateur.
Because, folks, poor though I am, tiny and unprofitable though my mortgage would be, simple as my other needs are.. there is NOBODY ALIVE who could have more skin in this game than me. And I need the chance to prove that to the bank.
More and more lately, I miss my Dad. I don’t know what he would have done or what he would have taught me in the process, but if he were alive, I would be safely housed. “Legitimate need? Doing your best? Got a rational budget? Okay, let’s figure this out.”
He was very staunch about facing hard realities and, working capitalist though he was, had many thoughtful conversations with his daughter about “from each according to his ability, to each according to his need.”
According to him, he loved that idea.
It was his favorite dictum about distributing resources, and he dearly wished it were realistic on larger economic scales. He worked in a world where it wasn’t useful, but he clearly wanted me to know that he honored it as an ethical guide.
He articulated to me how he used it as a parenting tool with his three gifted, demanding, and wildly different children. He said he’d never parent me the way he parented Older Brother, and Younger Brother was yet another proposition; he tried daily to treat each of us according to what he understood of what we each had, and what we each needed. He knew his perceptions weren’t perfect, and so it was a constant process to keep trying to improve his insight, as he kept trying to keep up with our development.
He explained all that nuance, admitted all that depth of thought and his practical limits, to his 11-to-13-year-old girl… in the late 1970’s. In some ways, he was way ahead of his time.
Through all the stormy years we had afterwards, I never forgot that, at root, he had that much faith in my mind and that much trust in my morals.
He’d be so proud of my diligence in all this.
Now, all I need is a reputable builder who’s up for this job, and enough working-brain-time to put all this medical and practical material together — preferably in the next week, due to the timing of the hard credit-check.
Neither is really in reach, but I’m here to keep trying. Wish me success!
Bonus Points
If I can get this done this summer, and recuperate in a safe home for awhile, then I’d like to put together a plan to make small safe homes all over these hills; I know people who can find the funding, and I know customers who’d be banging our doors down. It’s just that I can’t properly or legally use that program for my own benefit, so I must have my own home first.
Tell you what, I bet the whole process could be neatly documented and charmingly presented in an attractive book on the subject. It’d be one blueprint for a win-win way to help stabilize local neighborhoods, reduce blight, mitigate housing crises, generate middle-class jobs, stabilize local economies, reduce medical costs, and make many people more calm and content. All of which is economically positive in so many ways… and morally spotless.
I switched to a new insurance company that might provide dental care. I haven’t tried them on that yet, but I will. It’s on the agenda for this year.
They want to pre-authorize my main neurological med, Savella. This is the main med that keeps my pain under some kind of control most of the time. If it weren’t for Savella, I’d simply not have survived the past 5 years.
Somehow, the pre-auth requirement has thrown my pain specialist into a tailspin. He wrote a prescription (although I had refills) and mailed it to me, then asked me to come in to see him (2-1/2 hour drive, involving an overnight stay to be there in the morning, which is when his office hours are) in order to discuss this, before he’ll initiate the pre-auth paperwork.
I could get testy about that. It would be so easy.
What I did was refer, by date, to the first visit, when we discussed that first for 10 minutes. I guess his notes from that got lost.
This is where I stay off the computer for a day while I calm down, remind myself that it would not actually be in his best interests to throw me into a bottomless lake of fire, and it would probably not be in my best interests to beat him to it and kill him first.
When you have a brutal pain disease, and you have a med that works enough to let you have a life beyond fighting for the next breath and waiting for the lack of food and crazy stress hormones to kill you, and there’s a situation that threatens to take it away, the consequences of losing the med mean that life will descend into a level of hellishness that most people can’t even imagine. Thus, those of us who’ve found a med that works for us, enough to let us eat and move and think and speak — we get pretty intense at the prospect of having that med taken away.
This is not addiction. It never was. It’s true and valid need. Big fat difference.
Funny how it’s easier to believe when we’re not talking about narcotics, isn’t it?
> If you’re serious about managing the narcotic disaster in this country, you have to let yourself remember that both addicts and painiacs NEED TO BE PATIENTS. They both need CARE. Neither they, nor their doctors, nor their communities, are served by being turned into CRIMINALS.
> REHAB WORKS, when properly funded and designed. THAT is how you get addicts off of contraband drugs.
> PAIN MEDS WORK, when appropriately prescribed and used. THAT is how you keep pain-patients functioning as well as their diseases permit.
> There is some logistical overlap at times, but ADDICTION AND PAIN TREATMENT ARE NOT THE SAME THING.
> However, BOTH NEED TO BE MANAGED BY CLINICIANS, NOT POLITICIANS!
Okay, stepping off that soapbox. Feel free to copy/paste the whole blockquote as much as you like.
So, anyway, I’ve calmed down about my doc’s curious response to doing a pre-auth on my longstanding pain med.
This is really important: from here on, I’m talking about MY ANXIETY, not MY PHYSICIAN’S REALITY. This is pretty normal and natural, and I’m leaving it in as a straightforward demonstration of what my brutally nervous brain can do to in the grip of PTSD from decades of questionable care. So, here’s the anxiety-driven, defense-at-any-cost response. (For more on the reality, check my future posts on his doctoring.)
I remembered he’s a geek. More than that — he’s an ubergeeknerdyguy who’s been a high-end specialist for a very long time.
Geeks are brilliant in their particular slice of the world, but can be surprisingly insecure and nervous about stepping outside it. Also, sudden changes can be surprisingly disorienting to them. (Those of us with ANS problems can sympathize.)
Things that might rattle an ubergeeknerdyguy about this and set off mental alarm bells:
My med was covered before, but now it needs pre-auth. Why? /dingdingding!/
My diagnosis was wrong, and it’s possible that my treatment will change, but we don’t yet have enough info to decide what’s next. Feels like change is coming upon us too soon! Not enough information! /dingdingding!/
Winter. Nobody over 35 is at their best here in the winter. /dingdingding!/
Obviously, to those of us who don’t inhabit the intellectual stratosphere, the first 2 issues are pretty straightforward (1: Cuz American insurance is funny like that. 2: Doesn’t matter — stay the course until there’s reason to change) and the 3rd is just life.
To an ubergeeknerdyguy who’s accustomed to controlling outcomes that nobody else can bear to deal with, it’s too much uncertainty to handle at long distance.
So, I’m getting my documentation ready:
I’ve got another copy of the letter from the ins. co. explaining they just want pre-auth.
I’ve got the current formulary showing that Savella is covered.
I’ve updated my supplement matrix showing the changes for the winter, which does 2 things: shows I’m really working on this “being functional” thing, and that I’m taking my chemistry seriously, not being passive and expecting him to do all the work.
In fact, the last point is so useful, I’m going to link my matrix here for anyone to crib from:
Now my secrets are out! 🙂 You can now see exactly which brands I use and what I find that each thing does for me. (And, if you count up the number of capsules and pills this makes, you also know why it can take me over half an hour to get my pills down!)
Interesting points:
The first column shows changes (represented by a delta sign at the top). Docs LOVE being able to see at a glance what’s new and different.
Blank spaces are shaded out. This makes it obvious nothing’s intended to be there. (Common sense is not the same as intelligence, remember. Be as clear as possible.)
I put notes at the bottom putting it all in context.
My neuro supplements went down when I got my antioxidants dialed in to reflect the results of my blood tests. In other words, balancing my antioxidants really helped my brain!
My neuro supplements, along with everything else, have gone up to mitigate the brutal effects of cold and snowy winter.
This is not the time to make changes. Having said that, I’m not opposed to changes — just not now. (It’s good to explain, courteously and clearly, what your boundaries are around treatment.)
Detailing those changes tells the doc that I really do pay attention to what I’m taking in. I’m not a faddist; I’m diligent and determined to manage this as well as I can. Just from this one document alone, that’s reasonably obvious. Displaying this characteristic (or set of entwined characteristics) helps my doctors take me more seriously.
The real fun of this symptom complex: trying to keep others taking me seriously even when I realize I’m in such a panic my brain explodes. Woot!
Here’s my Doctor Appointment Optimization strategy. This is especially important for new diagnoses, new doctors, and any significant change or comcern you have.
– Between now and your appointment, keep a pad handy and note down anything you want to find out when you see the doc.
– A day or two before the appointment, set up your documentation. Lay those questions out so you have room to write the answers (in printout or on a notepad, whatever works for you.) Also, if it’s relevant or might be helpful, make a current Snapshot to show the doctor. Make copies of whatever science articles or studies you want to share.
– If it’s a first appointment with a new doc, also print out your current Timeline and previous Snapshots so he or she can absorb your info more accurately and easily. Put them where you can be sure they’ll go with you to the appointment. (Consider faxing them ahead of time, with a cover note asking to have them put in your chart. The doc can then review them ahead of your visit. There are benefits either way.)
– Let the doctor lead the appointment, because they find it easier to be forthcoming, but let them know you have a list to check against before leaving. They like that balance as a rule, because they want your need for info taken care of, but need to feel free to do things their way too.
– It’s your appointment. It’s their job to do you, and your case, full justice. Ask, and keep asking, until you feel you understand the answers.
– Write everything down, because the brain flips a switch when you leave the office and it’s amazing what you can forget.
– Get as many relevant printouts as possible before leaving.
– This is key, an enormous time saver in the long run: Go over your notes and handouts once you’re out of the office but before you pull out of the lot. Just take 5-10 minutes to sit down and go over everything, complete unfinished sentences, tie things together, fill in details you didn’t capture right away.
– When you get home, put your stack by your chair, get something to drink/eat, recharge your brain.
– Pick up your stack, pull out your computer or a pad, and put everything you’ve learned and acquired into a plan of action.
What are the most important things you got out of today?
What is the next thing to learn?
What is the next thing to do?
Are your next tasks and appointments on your calendar yet? (If not, do that. The ‘overwhelm’ tends to short circuit common sense. It’s pretty normal, so you might as well plan accordingly.)
– Once your calendar is updated, your to-do list is laid out, and you know the keywords you’ll need for further research, you’ve digested the appointment pretty well. So, get out your Timeline (which of course you have, or, if you’re new to having a chronic condition, you’re about to start) and fill in a new row.
The point of the pre-departure review is twofold:
1. It gives your brain exposure to the info outside the office, after that switch flicks in your brain, but before the info in all its rich detail gets dumped from your short-term memory.
2. With that second exposure helping secure the wealth of detail, it signals your brain to start working on creating networks between the new info and older info. This not only helps put your own situation in perspective and improves your base of knowledge, but it sets off a cascade of subconscious activity of a very helpful kind, destressing the situation and helping you get on top of your condition.
If this looks a lot like great study skills, there’s a reason 🙂 Chronic conditions require study so you can make better decisions on the basis of better understanding. This is definitely, fully, 5-star, hayull-yes, one of those things where the upfront additional effort (which honestly is pretty trivial) pays off a million times over downstream… in easier life changes, less trouble over choices, fewer complications, more time to spend on having your real life.
Speaking from way too much experience, it’s worth it!
May all your appointments go well and all your doctors be excellent.
Chronic pain patients are often called Difficult Patients, when the casual cruelty and reflexive contempt of medicine and the ignorance of other people grates too hard against our increasingly impaired ability to compensate and deal with it as calmly and “rationally” as we used to.
I’m less and less certain that casual cruelty and reflexive contempt are rational to deal with. Really, the *rational* thing to do is draw the line when professionals behave badly, no matter what the profession.
I’m increasingly certain that those who provide care, and have gone to all that effort to be trained and licensed to do so, should probably take on the burden of acting with more kindness and courtesy than those who pursue less intensive interactions with the wounded, disabled, and ill. Not less courtesy. More.
The rational thing for the professional to do then is to reckon that requirement into the cost — because respectful and courteous patient interaction saves money and improves outcomes, but more/higher administrator salaries do not. The data on that are very clear… though strangely hard to dig out on the second point.
I sometimes mull the mindframe I had when I was working as a nurse, which was deeply compassionate without being cuddly or fluffy. I was well aware that only one person was paid to be in that room and adjusted my expectations accordingly. But still, I think of the casual disregard of others’ humanity that defines so much of health-professional behavior, and wonder at the culture that reflects. It’s not that we have to do degrading things like shove needles and hoses into people, it’s that we won’t let them wear real clothes or secure their electronics or even eat real food, when they’re in our hands. We no longer even warm the gel.
Anyway.
CRPS patients are a special category of chronic pain patients: we may be dealing with a level of pain consistently rated as higher and more intense, not to mention more constant, than anything else — including childbirth, most cancer, having fingers ripped off — with the sole exception of terminal cancer pain, which is at the top of the McGill Pain Index. It’s horrible but true that terminal cancer pain doesn’t last as long.
So, we are a distinct, and distinctive, subgroup of the Chronic Pain Patient set.
On top of that, of course, the brain remapping and the neurochemical disruption of longstanding CRPS means that our central nervous systems are absolutely hair-triggered for terror reactions, which transmute into all sorts of other things when our intellect has to wrestle with the terror… because screaming and fleeing blindly into traffic shedding broken bits of furniture and wallboard is, somehow, neither socially acceptable nor particularly useful.
My old pain doc, Dr. Richeimer at USC Keck Pain Center, has a wonderful term for those whom lesser physicians call Difficult Patients:
Fragile Eggs.
Isn’t that perfect? Easily broken, and when broken, extremely messy and hard to clean up after. Treat gently. Treat extremely gently. Understand that you may have a mess on your hands anyway. Keep your cool, adapt on the fly as the egg rolls around, and stay gentle. There’s really no other way to handle it.
(Like many others, I love that man.)
So here’s the thing.
At the end of a crappy week (thick with grief), I had a Pap test (painful, intrusive procedure which is easy to do badly) scheduled to check for cancer (which is frightening) because I had a blood test come up funny that can be a sign of gynecological cancer (so there’s grounding for the fear.) I know as well as anyone that these things mustn’t be delayed, but I waited an extra week in order to schedule a long appointment so that the test could be done in a rational, CRPS-friendly manner.
Silly me. Turns out a “long appointment” is 15 minutes. That’s not a typo. FIFTEEN MINUTES is a “long” appointment.
I really haven’t been keeping up with the downward slide of the health care field below the level of the best-of-the-best I’ve had out West. I’m speechless.
Did you know it takes 5-7 minutes just to say hello and catch up on the case with a complex patient? Do you know what it’s like to have a speculum inserted into a body that is one long scream of pain already, and the tiny, cheap, but essential steps it takes to make that a wise thing to do? Did you know that good practice for intrusive procedures, especially for those with PTSD around their bodies (which includes most women, frankly) is to meet the patient while they’re still clothed and have them undress for the invasion-fandango after they’ve had a chance to be human, and not just one long scream?
I know, it’s crazy to think that patients are human. Forget I said that. I don’t know what I was thinking! Pfft…
I told the office twit who roomed me and informed me that it was a 15-minute vist that a Pap smear on a CRPS body was not going to happen in 15 minutes. Twice. She set up the torture implements, which did not include Lidocaine gel or a warmer, in the cool office, and told me to get completely undressed and climb into the gown she laid on the exam table.
She didn’t mention that my provider, the one decent and rational entity in that department, was running very late. I had to find that out for myself.
Sitting in the cold room, staring at the torture tray laid out directly in front of me, still fully dressed because I could not succumb to being led like a lamb to slaughter, I tried to calm myself, to get my brain out of the state of being hijacked by terror at the casual cruelty of being tortured into spreading this hideous disease into my viscera, and helpless rage at this high-handed and disrespectful way of being treated.
I tried to reflect that, clearly, a lot of women who came to this office for care put up with it and, knowing New Englanders, never even thought of complaining because that would be a sign of weakness.
I tried to tell myself that my provider would surely rinse the speculum in hot water before using it, but that thought was booted immediately. I know from prior experience as a healthy person that a plastic speculum does not hold the warmth, but it does hold drops of water as they cool off quickly, and the temperature of that object does not affect the temperature of the 60-degree gel they put on it.
So, viciously cold thing going into my CRPS-y body’s core. Then that pinching, twisting jolt as it snaps open in mucous membranes which are wired straight into my central nervous system as well as my visceral cavity. During a weather- and trauma-induced flare.
There’s just no way that can go well.
I sat there for half an hour, trying not to stare at the torture implements although they were unavoidable in that tiny space, feeling my brain run circles around itself, trying not to scream, feeling my capacity for verbalization and rationality bleed away in the chill.
I realized that, although I wanted to connect with my provider and use the time profitably at least in discussing these problems and finding out my ultrasound results, I couldn’t sit there any longer. I needed forward momentum if I was going to come out of this intact.
So I spent the next 8 minutes writing my provider a letter, left it on top of the Patient Update document I had brought in (which mentioned my prior interactions with the staff, ALL of which had been record-setting-ly stupid and unproductive), and I left.
I did NOT run screaming into traffic. I didn’t break anything on my way out. I politely commanded the twit to copy my letter “now please”, stood over her while she did it, laid the paperwork I’d created for my provider in a neat pile on her table, and kept my copy for my records.
Then I quietly walked out, smiling politely at my provider as I passed her in the hallway heading towards the nurse’s desk.
I made very little mess, for a fragile egg.
I got my documentation, but forgot my purse. There’s something very Isy about that. (I’ll go collect it next business day, and hopefully that will be the last time I have to see them.)
So, this weekend, I have to do 2 things: find a gynecologist equipped to handle complex patients, and put together my own gyn exam kit — with a suitable implement, lidocaine gel, and heating pads.
Sometimes, BYO* is the only way to go.
I may be a fragile egg at times, but I don’t like it and I don’t intend to live there. I can’t control the industry, but I can control what I walk into the room with.
♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦
*Note for non-native English readers: BYO is for Bring Your Own. BYO is derived from BYOB, which means Bring Your Own Beer/Booze, normally used in regard to parties (obviously!) BYO moved into common usage on its own as a handy verbal shortcut; it’s still informal, but not nearly as informal as BYOB 🙂
♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦♦
UPDATE from early March
I got my own speculum, the Pederson type (which is a bit narrower); found food-grade silicon sealant (which smells strongly of vinegar, but nothing more toxic) and applied it over all the contact surfaces and where the edges meet; and prepared a bottle of pain-reducing Emu oil with a bit of nerve-pain-reducing Clove essential oil added.
I called the largest and oldest gynecological practice in the area, and asked for the doctor with the lightest touch. I was a bit disturbed when a large, fit, square-jawed, brush-cut fellow walked in, but he turned out to be an angel. He was happy to use my speculum, poured quantities of my pain-reducing oil over that and his hands, and gave me a break halfway through the procedure to sit up, get my pain/panic response under control, and pull myself into reality and out of the shocky place.
I’m sorry to say that the Pap test itself was a lot like having burning coals shoveled into me and pushed around, so yeah, there is definitely some nervous system remapping that has already happened to my insides. (It used to be an unpleasant little scratching sensation, and no more.)
This doctor wisely asked for a copy of the funky test, which was my serum DHEAS level. I went to my other doctor’s and got copies and ran them over myself. I took a look…
The doctor who’s substituting for my allergy/immunity doctor who ordered this test dropped a very serious brick. THE TEST HE REFERRED TO WAS JUST FINE. I do NOT have an abnormal DHEAS value. It’s a whole lot more normal than the rest of me!
I wrote the gynecologist a note on the back to that effect, and let him know that he did the lightest, best possible job under the circumstances and that I’m grateful. He looked absolutely white and shocky by the time he left the room, so I think it was a pretty horrible experience for him too, and I don’t want to scare him off of treating other pain patients.
I got a Pap test out of the way and learned something important about the state of my disease. I’m being more diligent about my multivitamins and SAMe, the methionine-based antioxidant I use as my main antioxidant supplementation besides vitamins. I’m researching the least nutty, most promising pain centers near me, at Yale and Brown Universities (Dr. Pradeep Chopra is at Brown, so that’s probably first on the list) and this week I’ll be making appointments.
I guess every setback is really a redirection or a kick in the pants for me. I may have CRPS in my viscera (which would explain a few things) but I needed to get my act together about getting a pain doc anyway. My DHEA test was normal, phew, but I’ve been harshly reminded to double-check everything the doctor says. I’m seeing my usual doc at that practice soon, and I’m going to ask him to double-check DHEAS results to see if any patient has been left uninformed and unfollowed-up.
I took a few days after the Pap test to simply refuse to think about it, because I did NOT want THOSE pathways to go any deeper into my impressionable brain! Took it easy, watched and read silly things, ran errands with J, took loads of vitamins and drank plenty of water… then started researching the pain doctors.
This is my policy… strategic withdrawal if necessary, yes; pause, rest, reboot, definitely; but in the end, “Never give up! Never surrender!”
I collected health info on others for years. I’m what clinicians call “a good historian” — and in the health context, it means someone who can tell you exactly what happened to them and when it happened, and they turn out to be right.
This is fine… as long as I can keep track, and as long as the story is short enough for someone else to remember after a single telling.
They aren’t always paying attention.
This isn’t going to remain true for any case over a couple of years in the making, and certainly not for a case that even started out with multiple diagnoses: volar ganglion, tendonitis, and repetitive strain.
When I noticed that a doctor’s eyes were glazing 5 minutes into my recital of events, I knew I had to do this differently.
I started keeping a timeline. It was a nuisance to set up, because I got injured at work, and U.S. law doesn’t necessarily allow me to get copies of my records under those circumstances.
So I drafted my first timeline from memory, journal entries, and my datebook, and asked my doctor’s staff, as sweetly as possible, to please check the dates for me. They loved the timeline and were happy to do so.
As you can see, this is before I had a lawyer, and reflected my personal tendency towards information overload:
Click to link to the 3-page PDF.
As you can see, I decided to keep my timeline in a table. I found that to be the most natural way for me to organize the layers of information in a readable way. But then, I had just finished hand-coding and debugging about 21 pages of HTML tables in raw markup. Tables were easy for me!
To some people, a table of text just looks like word salad.
I can understand that.
There are other ways to organize information: brain maps, fishbone diagrams, bullet lists with nested lists, even labeled images linked together. Search any of those terms, or even terms like “information architecture” or “flow charts”, to look for ideas.
I took a later version of this to my first QME (QME=Qualified Medical Examiner, a consultant called upon when a U.S. insurance company disputes care in an injured-worker case.) Bless his stern and rock-bound heart, he gave me excellent advice. Here it is, as close to his wording as I remember:
“Leave out the insurance stuff. It’s not my department. It’s distracting, annoying, and clutters up the timeline for me.”
(I was not offended, because I’ve worked with a lot of hotshot doctors. I fully expected the brusqueness and just listened to the words for information. That information was pure gold.)
“In fact, thin this out a lot. I want facts, data, not suppositions or what you read. I want to know exactly what happened to you and what your doctors said or did. Everything else is filler. I’m a doctor, so doctors’ ideas are what I care about.”
(That was frank! And an excellent statement of inherent bias, which I really appreciated knowing up-front.)
“Take out the personal impact? No! No. I want that in there. It tells me how this really affects your life, and I should know that.”
(He was almost human when he looked at me then. It was a cool moment.)
“But I DO want the personal impact to be visually distinctive, so I can screen it out when I’m looking for the medical part alone.”
(That’s fair.)
“I’d also like to be able to find your work status more easily. This is a worker’s compensation case, after all.”
(Good point.)
That man should advise more designers. He’s retired from his medical career now, and I hope he’s enjoying himself immensely.
My next timeline, for my next QME, was much leaner and it distinguished between three key types of info: straight medical information, work status, and personal impact.
Click for the full PDF.
Did you notice how the hand images I wrote about before are referenced right in the timeline? This is a great way to build your case. The pictures kick the message of your disease progress and your needs right through concrete.
Incidentally, this uses mutually-reinforcing teaching principles: multiple sensory inputs, plus multiple paths to the same info, equals excellent retention. Your doctors will really be able to remember what your case looked like and what happened along the way, what worked and what didn’t.
Dr. F was pleased to see the table and thought it was basically a good idea, but looking at it through 78-year-old eyes was a different experience. He gave me his own feedback, speaking as someone who had gone through more medical records and had more problematic vision than anyone who’d looked at it yet:
“Yes, it’s nice that you picked out the work status, but I want to be able to see surgeries, x-rays, the really important stuff, just as easily. No, even more easily.”
I picked those out in bold and flagged them in the left column:
Click for a closer look at the PDF.
Before long, I learned to condense multiple entries so I could use one row for several visits that were about one issue, or where there wasn’t much change:
Then I saw a doctor who had more human sensibilities. He said,
“Why not use colors? I want to see surgeries and tests in different colors.”
I asked, “Do you want the different kinds of tests in different colors, so you can distinguish Xrays from MRIs from nerve studies at a glance?”
“No, no, that’s too much. I can read EMG versus MRI; I don’t want too many colors. I want the surgeries to really stand out, though. Put them in red.
“And I want to see the legal pivot-points, too, because that affects your case.”
Easy enough.
Click for pretty colors. subtly used, in the PDF.
Then the first page grew legs. Someone along the line said,
“One more thing. I’d really like to see your allergies and medical-surgical history immediately. If you could put that up front on this, that would give me the most critical medical information right off.”
That was a real forehead-smacker for me…
I used to be a triage nurse. I used to collect certain information on every patient I saw, regardless of age, sex, race, or what they came in with.
TRIAGE INFORMATION:
– Name, date of birth.
– Any medical diagnoses.
– Any surgery, with dates.
– Current medications and doses (if they recall), and what they take it for. (This fills in a lot of holes on the medical and surgical stuff — you’d be surprised what people forget. “Oh yeah, my heart stopped last month.” Good to know!)
– Allergies — and what the reaction is (because there’s a world of difference between something that gives you a stomachache and one that stops your breathing, and we need to know this if it winds up in the air or, heaven forbid, the IV line.)
This is basic. This is absolutely basic. It’s essential information that should be immediately surfaced on every patient’s chart. How could I take for granted that it would be easy to find in my medical record? The whole point of needing the timeline is that, after a couple of years, my medical record was a mess!
Also, after years of popping from one specialist/QME/consultant to another, I got tired of having to dig out the same demographic and billing information every time they had to generate a new chart.
I had a brainstorm: make the first page into a billing/demographic sheet, add the triage information, and start the table on its own page after that.
It all goes together on the medical chart anyway, and one of the unsung truths of medical care is this: make life easier for the desk staff, and they will make life easier for you.
Click to see how I organized this info. PDF format.
After all this time, I can put my whole history with this disease into one single document that totals 10 pages.
The first sheet has my contact, billing, and demographic info.
The second has my more-extensive medical/surgical history, medications and yet more allergies, and priority notes, highlighting my CNS sensitivity and emphasizing that cognition matters most.
The rest tells all the key points of 14, yes, 14 YEARS of injury and disease, in only seven and a half pages.
Here is the final result:
Every doctor, with one exception, who has seen this, has cooed — literally, cooed — with delight. They ask if they can keep it (I tell them to put it in my chart, so they can always find it. “Ooo, great!” they say.)
This one doctor looked at it, laughed rather sardonically, and said, “You spend way too much time on this.”
Clinical note: For the record, that is not an acceptable response. What clinician makes progress by dissing patients on the first visit? Right. None. The thing to do here is ASK; in this case, ASK how much time this patient put into creating the documentation. The answer certainly surprised this one.
I set him straight, in my sweetest tone of voice. I said, “After the initial setup, it requires only a couple of minutes of maintenance every few months. That’s it. Moreover, you’re forgetting that I used to be an RN and a software documentation writer; this information is easy for me to understand and easy for me to organize. If I CAN’T do this [gesturing to the document in his hand], you need to check for a pulse.”
He never sassed me again.
However, most of what I told him is true for all of us.
We are the subject-matter experts on our own bodies. Never forget this and never let anyone tell you otherwise, because they are wrong. You ARE the subject matter expert on your own life. Nobody else really knows how you feel or what you’ve been through.
It’s in your power to communicate that clearly enough to work with. It’s just a matter of figuring out how.
Once you get a timeline set up and put in the key events so far, it takes very little to maintain. I update mine before every key doctor visit — when I see a new one or when I need to see a QME or, of course, when I think a doc is losing the plot.
It takes me less than half an hour to update contact info, meds, and current entries, and I do that once or twice a year now. That’s a great effort/benefit trade-off!
Moreover, keeping a timeline has life-changing benefits besides simplifying explanations to my doctors. Every long-term patient can see how utterly transformative these changes can be:
The doctors take me and my case absolutely seriously from the get-go (or else it’s obvious right off that this person is never going to, and I need to move on. That saves time!) It stops arguments and attitudes before they even start. It makes me almost human in any good physician’s eyes, and that’s nearly a miracle, because, generally, they can’t emotionally afford to think of their pain patients as human. (This explains a lot.)
My medical records are a lot more accurate, because the providers writing them have this great cheat-sheet right there to help them stay on track and keep their facts straight. This has saved me more grief, bad treatments, misapplied care, getting meds I’m allergic to, and chasing red-herring issues with the insurance company, than I could ever count.
I can keep my limited brain-space free for handling the appointment and looking ahead, instead of trying to wrestle my complex history into shape. This makes my visits a lot more valuable to all concerned.
I consider my timelines to be worth roughly 1,000 times their weight in plutonium. A little bit of effort has paid off thousands of times over, and made it immeasurably easier to keep this messy, protracted, brutally complex case on track for nearly one and a half decades.
Now that’s a good trick!
Timeline Tips:
Put your name and the date on every page.
Put triage information (in second blockquote above) at the top.
Highlight surgeries and invasive procedures in bold and red.
Highlight tests and noninvasive procedures in a different color or style.
Highlight life impact, but keep it separate from medical info.
Attach the relevant doctor’s name to each procedure, diagnosis, or consultation.
Track adverse events.
Remember, this and all my blog work is under a Creative Commons Share-Alike Attribution license: do anything you want with it, as long as you don’t keep others from using it. I’d love it if you’d credit me with my work, but don’t let that slow you down.