Today, I learned (or re-learned) how much louder clothing speaks than my expression or manner.
I went out in my “hippie” disguise — a change from my usual “preppie on her way to a parent-teacher conference” disguise.
I like turtlenecks in winter. Anyway.
Today, in my shaggy green sweater with the red-and-purple geometric designs, people are *smiling back* and giving me extra time when my fingers don’t work.
I love my neat, clean, long-lasting basic wardrobe. (A bit boring, but well-kempt, smart, and will stick around forever. Kind of like my ideal partner.) However, I feel Indian cotton and flowy accessories in my future. I need to be responded to, more than I need to be respected — and possibly slightly annoying…
We grew up thinking happiness, joy, delight, etc., was spontaneous. It arose naturally from circumstances. If you had to go looking for it, or even put in the effort to crack open a door for it, it lost legitimacy. It wasn’t real.
Thank goodness that’s incorrect.
We know now that seeking the little joys has a cumulative effect that makes us stronger and more resilient. I’ve written about this before here 1 and here 2 (plus, it’s mentioned pretty often in passing), but it feels like time to mention it again.
There’s a social push, in some areas, to do like they do in zombie shows and batten down with All The Weapons and prepare to destroy all comers, because they will surely want to destroy you.
If that’s your jam, go ahead.
Social data and history shows that kindly communities generally weather hard times better. Everyone has different skills, and that only works well when skills are pooled in a varied group.
It’s like making sandwiches…
If everyone has peanut butter, you don’t have sandwiches, you have an impending plumbing problem once everyone has eaten it. That’s like everyone having the same set of skills or preferences — it’s just not going to work out well under stress.
If someone has peanut butter, someone else has white bread, another has whole wheat bread, another has slices of chicken, somebody shows up with pickles and mayo, another has lettuce and tuna, and an absolute star shows up with jelly and gluten-free options, then everyone gets a delicious sandwich.
Pooling resources is fun! And that’s how you get through hard times. Use your strengths and work with those who can do what you can’t. *
Scared of the zombies? One skill-set an amazing number of people around you have relates to tactics, strategy, combat, and martial arts. The US has been actively involved, as a major force, in wars around the world at least since the late 1980s, with only brief breaks before then. We’ve got lots of veterans, and they can build things, wire things, program things, bandage things, and cook, too. You’d be surprised.
Wait… How did we get here? I meant to write about how finding little beauties, stopping to soak up little joys, noticing and remembering what you like so you can go back to it — these all trigger “brain juice” in the form of neurotransmitters that help us regulate our minds and get closer to peace, poise, and sanity.
All of which is super handy when you’re picking teams to survive the zombie apocalypse. 🤣✨️
* Hot tip:
Disabled people tend to be overlooked. That’s absurd. Nobody is better at thinking around problems than disabled people, and we tend to have incredibly useful skills… because “disabled” is a misnomer. Most of us are highly able — we just have specific barriers, which we know all about. We can seek complementary skills and specify our necessary adaptations.
Come get us. You’ll be glad you did. A tiny bit of upfront effort, and then your whole project grows wings.
New series: Quickies. Short, practical notes, mostly about things to try for problems with CRPS, dysautonomia, mast cell & histamine disorders, etc.
Problem
I get what my grandmother would have called chilblains: cracks in the calluses around my feet and sometimes on my fingers. Nasty, uncomfortable, and — because they’re surrounded with thick walls — hard to heal.
Option
I’m an old nurse. I know a lot about healing wounds of all kinds. Nothing worked, at all …until I tried Ching Wan Hung, in the copper-colored packaging.
Ching Wan Hung: Different manufacturers but similar copper packaging
It’s a traditional herbal product with Chinese cinnamon, which smells a whole lot different from the tropical stuff we eat. It also has menthol, which I can’t tolerate normally, but is no problem for me here. I can scarcely smell it, so maybe it’s a dosing or production issue. Most herbal salves bring on menthol like a battering ram.
Usage
I squish it right into the cracks and holes of the sores, rub it in well, then put a dark sock over it for an hour. (It stains light colors.) Then I get on with my nap, or my task, or whatever. I put it on twice a day, before getting out of bed and at bedtime. I should probably use it more often for faster results, but I’m not very good at that.
It doesn’t work for everyone, just as everything else I tried, that did work for other CRPSers, didn’t work for me. It’s another option.
Sourcing
I’ve found it online at the usual places and at my local Asian/ international market, usually in little copper-colored tubes, which is more hygeinic than the larger tub you have to stick fingers into. It’s cheap for what it is, too.
You can ask for “Chinese burn cream” if you can’t remember the name.
Caveats
Use common sense (all my readers are extremely sensible, so of course you will).
If it brings up a rash or makes you wheeze, wash it off well and never use it again. Not for wounds that bleed readily or might be infected. Never use on bites, because mouths are utterly filthy and bite wounds need different care. If you can’t feel the tissues where your chilblains or non-healing sores are, see a doctor about them and follow their advice over mine. And so on.
I’m going to give organizing my mental database a try here. The aim is to pick one broad topic each month and cycle through them in a year. I’m doing it the way nurses and doctors are taught to do it: head to toe.
Physical assessments have to go from head to toe, every time, without exception. This makes use of the brain’s basic tendency to work in patterns. If you assess every patient from head to toe, every time, then the variances are easier to find (because your brain is so dialed into what to expect at that point in the pattern) and it’s a lot easier to get to a sound differential diagnosis.
If I go to the doctor with a sore knee, the doctor is still going to notice my level of consciousness, attachment to or detachment from my environment, track my gaze and whether the sides of my face are more or less equal, differentiate how much of my limp is because my knee hurts and whether any of it is because my balance is off (all of that is about the brain), notice my breathing pattern (lungs), become aware of blood- flow problems (heart) showing up in my skin, and checking to see if I’m “splinting” or bracing against pain or weakness in my abdomen (g.i/g.u. systems) and hips (ortho, right above the knee).
An experienced doctor does most of this in 1 to 3 seconds, because it’s a head- to- toe assessment every single time and they can just let their pattern-matching brain (which is powerful and primal) take care of it and send up a flag to their conscious mind if anything is abnormal.
The medical term for “head to toe” is “cephalocaudal”, which literally means “head to tail”… but humans don’t have much in the way of tails, and our bodies keep going for quite a ways after them. I’d love to hear from my Latin-knowledgeable readers what the term should be!
I’m recovering from a migraine, which is very on-topic, but I’m not yet up to writing much. I thought I’d introduce this new structure, which I hope will be a bit simpler and less overwhelming than “what am I wrestling with right now that I could usefully write about?” There’s so much to write about, it magnifies the intransigence of the empty page. (Writers know what that’s like.)
This is about the messy intersection of CRPS & the mechanical aspects of central nervous system dysfunction, and dealing with those effects.
I’m writing through the waunnng, waunnng, waunnng of a ringing headache. I’m hoping that if I hydrate, urinate, and (carefully) ambulate enough, it’ll pass faster. We shall see. Meantime, I’ll do my best to pass on some useful info.
The brain and spine are supposed to float in cerebrospinal fluid. We are supposed to stay hydrated enough to keep those sensitive tissues from grounding out.
We have 2 kidneys – each one capable of filtering twice the water we actually need – as a practical accommodation for the fact that, throughout history, most water was filthy and needed lots of filtering.
We have 4 times the kidney power we need for a busy, messy lifetime. We’re supposed to use them! The more we use them, the healthier they can stay. They love to do their job.
When we’re properly hydrated, our brains and spines can float comfortably in their spaces. When they float comfortably, they have plenty of shock absorption protecting them.
Spinal care
Dr Faye Weinstein taught me an important part of brain & spine care.
I had too little cartilage in my knees, so I had developed the habit of dropping into chairs instead of using my legs to lower myself neatly.
She hated that. She visibly flinched, and one day she finally cried out in audible distress, “Stop doing that!”
I stopped doing that.
Just as she had predicted, my baseline level of misery became less.
Once I was out of the habit of dropping into chairs, then, when I did it again, it caused headaches and sometimes back pain (depending on my hydration, of course). I was no longer used to enduring this as part of my daily quorum of yuk.
That was (checks watch) over 10 years ago. My brain and spine, oddly enough, haven’t gotten any younger since then.
Yesterday (after a couple of days of being “too busy” to hydrate properly), while I was turning to admire something across the street (a boat or a building; I forget which)… I stepped off a step I hadn’t noticed. One step down, caught myself, barely stumbled, no harm done. Massaged my neck a bit, to ease the slight jamming on one side. In my formerly healthy system, that would have been that. Probably would have forgotten about it instantly.
But now is different.
It took 10 minutes for the icky feeling to set in at my low back and back of head. It took a little over 2 hours for the whole brain-fog and uncontrolled body pain to take hold. Chronic CRPS really is wired into the whole neurological system, and one of the hallmarks is how the spine takes on an anti-life of its own in the face of any signs of disrespect.
Clearly, my spine felt seriously disrespected.
Content warning – skip this description if you’re squeamish about pain:
We know that I have no effective pain control left to me, with genetic tweaks making narcotics disgusting (they make the pain worse, cause untreatable nausea, and trigger horrific mood swings), and mast-cell activation making NSAIDS unbearable (they cause a soft-tissue-wide inflammatory pain, making it feel like shards of hot glass are hammered into all my cells).
So, how to approach this?
There’s a super-concentrated lemon balm extract that helps calm down inflamed nerves. Lemon balm has been used to calm nerve inflammation & pain for, approximate thousands of years.
Since all the nerves coming out of my spine are feeling very hot right now, I’m taking that about every 8 hours.
Note: check this against your meds, especially with GABAnergics. Ask your pharmacist to check their standard herb-drug interaction charts.
Pain salve on my spine and up my neck before bed, and also on arms/ shoulders and hips once I tried to sleep, helped noticeably.
It was a rocky night, but I’ve been getting as much water down as my tummy will tolerate and, now that my kidneys have been flushed 3 times, the headache is noticeably easing.
Conclusion
We can’t be alert every second. Our senses are so distracting at the best of times. Finding ways to manage these impacts is unspeakably important.
Long-term pain patients tend to get self-concerned to a degree that could be obnoxious normally, but it’s a legitimate self-care attribute in a life where one wrong move or one wrong exposure can destroy weeks or months of work.
Image by neurollero on flickr, CC share-alike attribution license.
One benefit of this self-attention is learning how to manage and mitigate the problems that arise by catching them early, and sharing the info in the hope that it’ll do some other painee or their caretakers some good. We have to learn from each other. Nobody else is as qualified.
I’m working on building up stamina because being a blob doesn’t agree with me.
I had one of our rare, hard-won, absolutely stunning neuro physiotherapy sessions yesterday. It usually takes time (days or even weeks) for my body to embrace the resetting, but this one is showing up fast.
Until last week, walking a bit too far would wipe me out.
When I was well, walking lifted my spirits and calmed my mind, and “too far” had more to do with comfort & convenience than anything more pressing.
For most of my illness, walking helped in the aggregate – if I kept it up, I did better over time. It was good, and I was glad to do it, but…
I’d forgotten, until today, just how lovely it was possible to feel after a good walk.
Yes, I’ve overdone a bit, and I’m open to the idea of staying in tomorrow & taking it easy.
I just… I haven’t had a workout high in… dear heavens, I can’t even remember. Decades, possibly.
Must remember to send this link to my physiotherapist. She’ll be:
A. Over the moon for me.
B. Reminding me to drink a lot of water and put my feet up for a bit.
It’s hard to keep it all in perspective – to celebrate this properly, without falling into the old trap of ignoring all the ongoing work it took to get here; to keep it up & stay honest about the jungle of limits I still have to negotiate.
Good day, though, eh? Really, really good. My heart is as light as the feather of Ma’at…
I’ve been chewing over something for awhile and recently realized that it might be time to apply that much mercy to myself. It’s a more coherent, whole way of thinking about what I discussed in some panic in my previous post.
Complex chronic spoonies tend to drive ourselves hard because we really have no option (the exhausting, but relevant, internal chorus of “adapt or die, figure it out or eff off, push through or give up, fight or fall” is inescapable) but does it need to be so ubiquitous?
A lot of these posts have been oriented on finding light through the cracks, on putting life itself into center stage somehow. I think I’m cooking up a new way of doing that.
The most basic of basics
Many years ago, when I was working as an emergency nurse, I realized that (despite the hype & excitement) our job was fundamentally simple: give people another chance to get “it” right.
Whether “it” was keeping up with their meds, staying off of whatever was poisoning them, choosing better company, finding the healing path that worked for them – whatever. There are fewer “its” than their are people working on them, which is why we are never the only one with our struggles.
That made more sense inside my head. Sorry.
People wind up in the ER because something bad happened, and usually human ignorance, stupidity, or violence was involved.
That’s not about blame. People don’t always get to choose their company or can’t always bear to be alive without some kind of buffer between them and their situations. Even if they did do something colossally daft (like the rich kids who decided to cut out the middlemen and drive 350 miles to buy their drugs from the distributor; 4 came down, 1 eventually went back), it’s not right to require mistakes to be terminal if they don’t have to be.
Of course people with heart disease should take their meds even when they feel fine, and get periodic blood tests to show that it’s working. Of course people with diabetes should keep an eye on their blood sugar and stay on their meds. Of course primary care when you first get symptoms is better than going to the ER when you start to fall to pieces… but it’s awfully hard to find a primary doctor these days.
Life is complicated and increasingly expensive. ER work really shows that.
Anyway, I saw our job not as holding back the sea with a broom (as some do), but as giving individual people a chance to figure out how to do things better. Lift properly. Drive sensibly. Stay off the hard stuff. Find an appropriate doctor who’ll listen – and then talk with them.
Nobody likes to be told, so reciting these mantras to them doesn’t often make sense. Oddly enough, it can be a lot more meaningful when you’re meeting their worried gaze as you administer the medication or fit their c-collar or go over the x-rays with them. Or tape and dress the wounds in their wrists.
There is so much we don’t control… sometimes we just have to remember what we could control, and how to put that in reach. It’s not easy, but it’s often very simple. When the universe is dropping its big hammer, where do I need to be when it lands? Under it? Or can I get off to one side? What will I have to let go of in order to get out of the way? Is it worth it?
The answers to this aren’t always obvious, and “worth it” to some is not the same “worth it” as for others.
What that looked like in practice
We had a lot of repeat customers. Some of them I wound up zipping into body bags, because what it took to get out from under the universe’s hammer was either too far out of reach or not ultimately worth the effort of letting go of what they were clinging to. They mostly didn’t want to die, but it wound up being too hard to do what it took to live.
I’ve got to respect that. It’s not for me to judge.
Some of them I saw come back just for ordinary bump-and-owie stuff, showing me the healing scars (inward or outward) of their old struggles. There are no words for the sense of sunrise I felt on seeing them. It made the rest worth doing.
It was all their work… but it was up to us to give them another chance to get it right.
My chance
I absolutely love to work. Being useful and productive is the bomb! If it weren’t so important to me… well, I probably would not have come down with CRPS, which stemmed from relentless overuse injuries in my case. I could not take a break to save my life. Whatever it was, I had to jump in with both feet, arms flailing and shouting “incomiiiiing!”
I imagine I could be pretty tiresome that way. Belated apologies to my friends and colleagues along the way!
I’ve been wrestling – for years (how embarrassing) – with recognizing that having fun… recreating… seeking diversion instead of merely a change of work… I’m not even sure how to put it… but that loose, apparently useless, seemingly non-productive use of my time, is really good for me.
It lowers my stress levels. It reduces my pain. It raises my spirits. I don’t know if it gives me back any of my lost abilities, because I find it incredibly hard to do and have never been able to hang onto the easy-going vibe long enough to find out.
What with one thing and another (I’m an American living stateside in January of 2025; IYKYK) I have a powerful inward pull to go somewhere glorious – and affordable, thank you very much – and simply muck about enjoying the diversions. Play tourist for once in my life. Soak up pretty colors and different sounds. Be warm every single day.
And, if I get bored or don’t like it well enough, simply go somewhere else.
At this point, a lot of places are more affordable than the U.S. (more on that later) and, for all the challenges of travel in this body, I do plan on doing nothing but recover and enjoy myself for a good while afterward.
…It’s a weird idea, honestly.
Good thing I’m used to maintaining and cultivating relationships via the internet, after a quarter century of having to do so. It makes love more portable.
It’s still a weird idea. Wherever I go, I still bring myself along, and I know I’ll have to leave my compulsiveness behind with my snowboots. That’s unnatural, but I’ll learn.
Learning to let go of that deep attachment to being productive and useful is not the same as not being productive and useful – but it could give me time and space to heal my much-clobbered systems.
That might be the point.
Rest and play is widely regarded as essential. I think that’s the “it” that I need to work on getting right. Get out from under the falling hammer of overdriving a broken system.
I’m likely to post more often, about littler things, and to mask less about the impacts of my illness and circumstances. I’m hunkering, and inviting you to join me.
Today’s topic is about a beautiful thing.
Olive oil is proof that the Earth loves us and wants us to be comfortable.
Sadly – and, I’m sorry to say, despite marvelous advertising and gorgeous labels – most of the olive oil you can buy is mixed with other oils, whether or not that’s legal or whether the labelling indicates this. This dilution is so integrated in key parts of the industry that there’s not much hope of stopping it, but honest people keep trying (https://www.foodnavigator.com/Article/2024/08/08/olive-oil-fraud-increases-in-europe).
However, it’s a big world and artisanal food is becoming more accepted and appreciated. This creates light between the cracks, so it’s still possible to get 100% olive oil that’s not diluted with something unfortunate, as long as you have a sufficiently sensitive laboratory on hand to check it with.
I do. My analytical laboratory looks remarkably like a reactive, chemically over-sensitive, mast-cell-activated human system which I’ve been working with and paying attention to almost since I was born. It’s expensive to maintain but easy to move. It goes everywhere with me, so I can always check what I eat, drink, and breathe – whether I like it or not!
It’s not always clear about the details of what it reacts to, but if there’s something at all whacky with whatever I’m taking in, my system will generally let me know in anything from moments to hours.
My body can’t stand any rancidness and it screams its head off at oils that should, theoretically, be fine – as long as they’re highly processed. Canola and deodorized oils are pure hell for me, triggering pain like ice-picks swinging into my arms and stomach.
Certain kinds of refining techniques make otherwise innocent oils do likewise, although they might fool other, more ordinary labs into reporting that there’s simply nothing amiss. Technically, there isn’t, and an ordinarily healthy body would agree with that. Lucky things.
My body has its own criteria and levels of accuracy, levels which remind me that some physiological events are triggered by molecule-sized exposures (as are hormones and immunity, even in healthy systems) rather than by mouthfuls or serving sizes.
Experience has taught me that it’s cheaper and easier to pay attention to my built-in laboratory and its reports, rather than try to convince myself it’s imaginary and the marketing, labels, and purported 3rd-party tests must be more correct than my own body. Nah… my body is a better guide about what to do for my body.
Where to start
The easiest test of olive oil’s purity is whether the oil smells olive-y. (If you don’t want olive-smelling oil, might as well use something else anyway.) I always start there.
From much experimentation over the years, I’ve found that olive oil that’s 100% Californian is pretty reliable. Almost anything can be grown in that region, but the market for adulterants (like deodorized hazelnut oil, commonly used in the Mediterranean) is hotter in their more natural state in California. I can’t really imagine California nut farmers – a proud group, not to mention bright & as profitable as possible in a drought-torn land – processing their oils into bleah and selling it for pennies on the dollar. Nope, they’ll take top dollar for their good nut oils, thankyew!
Olives are probably better-suited to California’s arid weather than thirsty nut trees. So, apparently, it still makes financial sense to deliver all-olive olive oil.
Naming names
I’ve found 2 brands of olive oil that currently work for me. There used to be 3, but one got hugely popular and ramped up their supply to meet demand and draw down prices, and (for whatever reason – I’m not making any accusations) their oil started hurting like heck.
Oil #1
Paesanol is a family-grown Italian oil. It has a slightly buttery mouth-feel with an olive-rich scent and a glorious flavor. The organic version is as good as a pain pill, actually knocking back the pain and confusion for about 4 hours, or even breaking the cycle. The price varies considerably through the seasons and right now it’s at peak price. (I stop paying attention when it gets over $30/bottle). The price should come down again when the new season is bottled and shipped, probably pretty soon.
It doesn’t have all the usual tags and certifications that a foodie might look for. I live in a great growing region and I know that good farming doesn’t always mean being willing or able to handle the extra paperwork that certificates require. Whatever its status, it works like a charm for me and I love it.
Oil #2
My go-to (now that Paesanol is out of reach price-wise) is Cobram Estate, a 100% Californian olive oil from an area I used to live in. It’s very good, though it doesn’t have quite the lush personality of Paesanol. Slightly peppery, which I like (because I can’t have real pepper any more). It marries well with other flavors, making it a wonderful base for simmering with garlic and herbs and making flavored oils with, topping soup with, mixing with veggie mash for those of us on low-residue diets, or splashing on eggs or salad or bread or anything else. Excellent all-arounder.
It helps a little with the pain, but, most reliably & importantly, it never makes it worse. That’s the key, really.
Afterthought
As food prices rise (amidst record profits for agri-biz and food suppliers, hmm), I expect to have to revisit this and try some more beautiful bountiful olive oils. I hope I can find a few that settle well and don’t hurt. It’s good to have options. 2 is not a lot of options.
Most people want a reasonable life: reasonable effort should result in a reasonable income, so they can keep a roof over their heads, feed and clothe their kids reliably, and be able to get out once in awhile.
This is increasingly difficult. That’s not reasonable.
As for me, I want to be, not only safely housed and fed, but also in not-too-much pain so I can get a few things done that help, cheer up, and inform & amuse those I care about.
I headed to psychotherapy after texting, “I’m on my way. I’ll see you in person today, barring the unexpected”
I was feeling a bit cautious, because a couple hours before, the thought had come to me, “when things get hectic, trust your training.”
What training? Was I about to have a series of intrusive thoughts harking back to the times I’ve had to file restraining orders, one of which magically disappeared and I had to flee the area – right before Christmas? I hoped not. Martial arts training has certainly come in handy, but come on…
No, no intrusive thoughts, but I did wonder which set of training I should have in mind.
A few miles down the interstate, I saw a pickup truck stopped dead, and a sedan facing it.
People were only just getting out of the truck. I put my flashers on and pulled in behind.
I definitely trust my training in this kind of situation. I put my anxiety to one side and sailed in.
The only person to worry about was a littlie in the back of the sedan. Had spontaneous pulse – a good one – and respirations. He could speak, to the limit of saying, “I want my Mommy” (sound of heart-strings tearing), so I checked his spine at his neck. It was there, but not quite right. Once he could speak more, he told me his neck hurt where I touched it (I’d been holding his head & neck stable since I felt it). As I told the fire department medic later, “on me, it’d be a chiropractic adjustment. On a littlie that age, I’m not sure.” He nodded and sent his buddy in with a pediatric cervical collar.
Littlie’s mother was on the phone the whole time with him. So much love swirling around in that car. I told the Dad that I noticed it, and that it’s healing.
At each stage – or rather, just before the next round of excitement – I explained to Littlie that there would be more people, highly trained people who really cared about him being okay. Let him know roughly what to expect at each stage. Coached him to go along with things as well as he could. When the fireman asked him to squeeze his finger, he squeezed my hand instead (sound of heart melting).
I could see most of my words going over his head (as expected), but I could also see the sense of reason and structure calming his exhausted and shocky brain so he could tune in a little more.
I grew up in a musical household, so naturally I hummed pretty little made-up tunes and it visibly calmed him – and possibly his parents too, a little.
I’ve been working on learning how to stabilize a shocky system for 25 years, on top of my trauma nursing work. I’m only a patient – and a nerd – but still, I have lots of good training. I trusted my training in that, too.
I gave his mother my number right before the fire department and EMTs rolled up. I think it was a training day, because there were 7 or 8 more people there, one of them a cheerful charming know-it-all (every team needs one of those) who got the best responses out of Littlie.
I let the kid know I had to go but his Mommy would stay on the phone with him and he’d be cared for by these really nice people. Told his Mom I loved her kid and he was terrific (sound of heart-strings pulling).
Once his c-collar was on (definitely a training day; I helped get it positioned and sealed correctly in the end) and they had the gurney ready, I realized I had to stand up. After perching my crippled butt by one hip on a steel door frame for half an hour. In front of people. Specifically, a total of 9 or 10 fit, athletic slabs of beef (-cake) no less than 10 years younger than me, and most of them half my age.
This was not going to be great for the ego, but I knew I could get a laugh out of it.
So I used both arms and every available leg (which was slightly less than 2) to lever myself upward, saying, “I’m an *oooold* trauma nurse” by way of cover, and squirmed through the kindly, protective testosteronic press and into fresh air.
I signed off with everybody and retreated to my comfy car.
I called my psychotherapist and said, “Remember what I said about ‘barring the unexpected?’…”
We had a phone session once I was safely off on a side street and in a proper parking space. She was full of commentary about how I applied those psych skills and met psychosocial and informational needs appropriately, as well as the nursey stuff. So yeah, that was good…
… because my brain was churning constantly about every single moment and thought and decision for an entire hour. Looking for a fault. Looking for something I’d missed or where my training had lapsed or been forgotten. Cycling through, over and over, looking for any lapse.
This used to be how I improved my skills – look for errors, even tiny ones, and figure out how to prevent or avoid them in future. Now, it’s just my ADHD brain torturing me.
And computer says Nope. Failed to suck. I’m pretty sure I failed to suck. That’s a relief.
I’ve been thinking about it pretty much nonstop, but rather than worrying myself woolly, I got an organizing thing for my car and picked up some food. Both of these are calming, grounding things, perfect for pulling my adrenaline out of the stratosphere.
Then I crawled home and had fresh corn and gluten-free carrot cake for dinner. It’s good to have a little sweetness when your body is still convinced the world is full of excoriation.
I’ve had no calls from them and I don’t expect one. They’ve got to be absolutely wrung out regardless of how things went. The kid comes first, and then comes their own care and self-management.
They don’t have to think of me ever again: I know how shocking and painful it could be to revisit the moment.
I’d love to know. I hope like crazy that the kid came out of it OK. I never got to follow up with patients when I was a nurse (because confidentiality), and I’d sure appreciate it if this family wanted to give me a heads-up just to soothe that old itch.
All that being said, I want all you non-nurses to know that they don’t owe me one word of contact or one moment of concern. I was in the right place at the right time with the right training, and I trusted my training. That’s what we do.
They have the hard part: figuring out next steps with a shook-up and possibly injured Littlie who was going home early because he was already ill.
That kid was having a rotten day.
I sure hope it got better.
Forestalling future problems
I don’t have a jump-kit for my car. That could be a problem in the future. I was lucky this time because all I needed was my brain, arms, hands, and voice.
It’s probably the 6th or 7th accident I’ve stopped at and I really do know what’s needed at the roadside – and it isn’t much. I used to get confused by the fact that I didn’t have a stethoscope, oxygen on tap, i.v. gear, and All Tha Meds. Once I’m on scene, though, it gets very easy.
Any blood or, indeed, anything wet? Nitrile gloves, packed up in pairs and stowed in a closed outer pocket to keep them clean & dry and easy to get on.
Heaven forbid, does anybody need CPR? This very rarely happens, but when it does, I don’t want to have to dig for the needful. I physically can’t do chest compressions (though I can coach any able-bodied person properly) but I can darned well use a mask with a one-way valve as if I’ve had years of practice. Years. You don’t have to have that (the training has shifted away from doing rescue breathing) but I feel that I do.
Pressure dressing? Kerlix. Sling? Kerlix. Wound cleaning? Kerlix makes a great sponge. Wound wrap? Kerlix. Piece of clean water-resistant paper to slap over a bubbling wound? Wrapping off a Kerlix.
So, plenty of Kerlix.
Road rash? Plenty of saline rinse (and a Kerlix) then a petroleum dressing to stabilize the damage until the ER can do a better job.
And possibly most essential: disinfectant cleansing towels, individually wrapped and big enough to grab. Those get used before if there’s time, during if the patient wants cleaning up, and definitely afterwards.
Because allergies & neurological reactivity, I stick with ethyl alcohol 70%.
Secure the mess. A gallon-sized zip bag or 2 for garbage and wrappings. Having a garbage bag is one of the things that separates rescuers from ego-trippers.
Oh, did I say that out loud? Sorry. I don’t want anyone not to stop & help… I just wish that, if they’re going to the effort of bringing gear, they could pick up a bit. Seeing blood and mess is not good for survivors & passers-by.
I got all these online for about $10 each, and also got a clear bag (with outside pockets) to put the kit in.
I’ll keep backstock at home.
What I don’t carry
Blood pressure readings, stethoscopes, and pulse oximetry are at-home and in-hospital concerns: we want to know if what we’re doing is working over time and refine our understanding of the body’sfunctional state.
In the field, the main issue is not whether the patient has rales or a murmur, but whether the lungs and heart are keeping them alive – a much simpler, larger-grained issue.
So, these tools might be nice to have, but for a noodle-noggin like me, they’re an added complication and a bunch of expensive equipment to lose at the scene.
In the field,
You need to keep pulse and respirations going,
the spine stable,
make sure the inside stuff stays inside
and in place,
and (as much as possible) the outside stuff stays out – or at least doesn’t move much where it’s inside the person.
And that, ladies and gentlebeings, is Advanced First Aid and Basic Life Support in a nutshell. You’re welcome 😊 Now go get that training… please?
I wrote the start of this for a fellow spoonie today and realized it’s a good starting point for a subject most people find overwhelming: reading medical science when you’re starting off as a non-scientist.
The article I cite first is a good example to start with, because it’s written well and has passages of clear English to work with. So…
I suggest reading the abstract and introduction. After that, just skim the first sentence of each paragraph, since (in science writing) that tells you what the paragraph is about.
If the first sentence makes no sense, skip that paragraph.
If you can figure out the first sentence, glance at the rest of the paragraph to see if there’s any more to glean. If not, move on..
It’s a skill
Reading science is a skill, and skills take time to master. That’s expected! Share what you glean with your doctor and ask them to help you understand it better.
Honestly — this isn’t to puff myself up, it’s just the nature of patients to dis themselves, so hear me out — if you can read my stuff and make out half of it, you are plenty smart and literate enough to start reading science. It’s just work and time, and the time will pass whatever we do, and the work will get easier with time. We just have to take care of ourselves and pick our time, when we’re chronically ill.
Using the right amount of honey
Doctors might give you attitude about comparing your Google search to their medical degree, but that’s not what you’re doing: you’re studying up on your condition, which is wise, and you’re expanding your info base on this thing that has imposed on your life, which is survival.
So, feel free to correct them sweetly, and don’t be afraid to pour some admiration on them if it helps them to re-focus on your information-gap.
The point is not who knows more overall. That’s not in question. When you talk to your doctor, you’re talking to someone who had to memorize, for instance, the Krebs cycle (here’s a partial explanation: https://www.medschoolcoach.com/the-krebs-cycle-mcat-biochemistry/) — so, yes, they have a depth and nuance of knowledge that’s nearly impossible to replicate without going to medical school.
They like having that acknowledged, because they take a lot of painful flak for not knowing everything about everybody’s illnesses all the time, and they need to know that you know what an effort they made to be able to work as a doctor.
So, it’s good to acknowledge that enormous effort.
Then they are usually able to hear you when you clarify that you’re not arguing with them, you’re trying to improve your understanding of this thing that affects you so profoundly. You trust them to help because of their knowledge.
Trust. Help. Knowledge.
These are keywords because they are core professional values for most doctors.
They’re important to acknowledge, and great to invoke and rely on.
That said… if you can’t rely on these characteristics in your doctor, even after you tell them that that’s what you need, then it might be time to find another doctor if you can. These core values are far more important than whether a doctor has good social skills or a good handshake.
When all is said and done, guess who has to live (or not) with the outcomes? It’s you. While the doctor is the subject-matter expert on the medical info around your condition, you are the subject-matter expert on being in your body and dealing with the fallout. There’s a degree of respect that should go both ways, though modern practice makes that hard.
The key to reading science is realizing — or at least, going ahead as if — you’re perfectly capable, and just need to practice. Science is written by humans, and you’re a human too.
1. You are a perfectly sensible person. If you’re reading this, you know how to read (or access translations from) English; also, you have access to a whole world of dictionaries. MedlinePlus is especially helpful in explaining concepts and helping us learn to read medical stuff.
2. Not all scientists can write well in English, and none of them write in English all the time. That’s okay. They went to school for a long time to get extra vocabulary and learn to do what they do; good for them. They’re still people, and they have to write in English at least some of the time. That’s where you can come in.
3. You can read the English just fine. Trust yourself and take time. With practice, you can learn more lingo over time, and get better at reading more science.
Just work from what you can understand now, and let that grow over time. You’ve got this.
Choosing credible sources
While you’re learning to read science, start where you can and work from there. As you get more confident and your understanding grows, you’ll learn to be choosier.
The gold standard for science info
When learning how to assess science, you’ll hear a lot about placebo-controlled, double-blind studies and that method is often important. This method of science gives us more reliable statistical probabilities about whether something will work in a certain situation. The statistical probabilities become reliable when several thousand people (“subjects”) have been tested, probably over many different studies.
With rare diseases, this is obviously pretty unlikely, so we have to work with less scientific certainty. C’est la vie.
Statistical probabilities have more limited value for patients than doctors, because we’re individuals, not pooled data. There used to be a phrase used in medical school: “Statistics mean nothing in the case of the individual.” This has gone by the wayside a bit, but it’s still true.
We may have to cast our nets further afield, because we’re looking for clues that might help us, personally. Be aware when you’re doing that, and put those science reports in your mental “hmm, maybe” folder.
I showed a case study that had a marvelous impact to one of my best doctors. He said to me, “If I could put that effect in a bottle, I would. It worked for that person, and we have no idea why. We do know that it doesn’t work for all these other people. Everybody’s different. Figuring out how to apply one thing to help a lot of people is our holy grail!” Lloyd Saberski, MD.
And that’s why doctors rely on the pooled data gathered from the scientific method. They want to help as many people as possible with each thing they try. Otherwise they fear they’ll spend too much time chasing rainbows.
We patients have to find our own rainbows, just as we have to count on our doctors to keep an eye on what’s statistically worth trying. It really is teamwork, and we both need to do our jobs.
What’s peer review?
Before you give a study to your doctor, it’s worth checking if it’s from a peer-reviewed journal. Don’t expect them to put too much stock in it otherwise.
Peer review means that other people in related fields have checked it over for sanity and validity. This is important for us patients, as well as the doctors who rely on the information.
You can Google whether the journal your article was first published in is a peer-reviewed journal. JAMA, BMJ, and the Lancet are all reliably peer-reviewed.
The value of literature reviews
Then, after a fair amount of studies have been done on a topic, there’s usually a literature review. This is when a qualified scientist takes a close look at all the studies, throws out the ones that were badly designed or poorly run (because bad technique creates bad data. “Garbage in, garbage out”) and writes an overview of what the current good science says.
They also discuss the strengths and weaknesses in the data, and suggest where future science funding could go, in light of the science so far.
Literature reviews are wonderful places to improve your knowledge of your disease/condition, expand your vocabulary, and get a lot better at understanding what goes into the science on your condition in the first place.
For instance, it used to be widely believed that most people with Complex Regional Pain Syndrome had had traumatic childhoods. (“Blame the parents” LOL.) There was a literature review done on about 30 years’ worth of studies, and it turned out that almost all of them were so badly-designed, poorly run, and calculated with so much bias, that nearly all of the studies had to be thrown out!
This taught me very important lessons:
– Just because most people say it, doesn’t mean it’s right, even if they should know better. This is an excellent attitude to have while reading science.
– Methods matter. You’ll learn over time how to sense whether the methods used are appropriate to the topic studied. The wrong method can lead to truly bogus results. The method has to fit the material.
– People lose their minds when they think about pain, as well as when they think about childhood trauma. In practical terms, this means I have to approach all normal (non-CRPS) people’s reasoning about my condition (which is characterized by relentless agony which a non-CRPS’d brain cannot even conceive of) with compassionate criticism. They do not know what it’s like, nor how to live with that pain and still think rationally. They’re not able to know. I don’t want them in a position where they do know, because that’ll mean their lives are as battered as mine is.
Therefore, every word they say has to be filtered through my awareness of how their minds get lit up by unreason, when they think about my pain. This, believe it or not, is perfectly natural. (Look up “amygdala hijack” for background on this mechanism.)
I survive because I’ve learned to substantially displace or ignore one of the most powerful primitive signals in the human body. That isn’t natural, and nor should it be.
These scientists mean well, without question. However, their logic is necessarily fractured when thinking about this, because they lack my tools for facing it. I need to dig into their data and methods before I can buy into their conclusions.
That’s good to know!
The conclusion of that literature review? CRPSers are likely (not guaranteed) to have had relatively eventful lives. Whether the events were traumatic or wonderful wasn’t relevant to our probability of developing CRPS.
In other words, we live in interesting times!
Where to find science to read
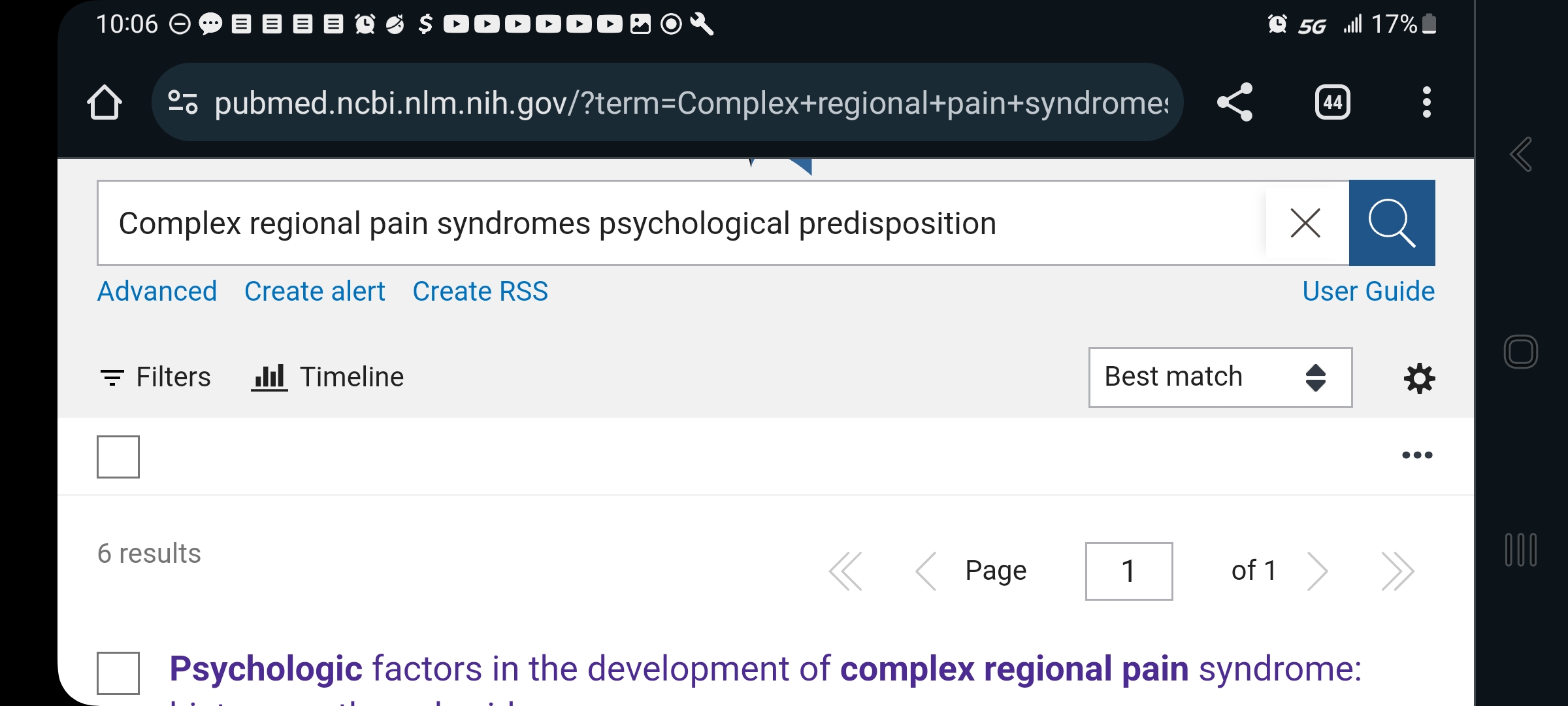
Google pubmed, and you’ll find the National Library of Medicine (NLM) division of the National Institutes of Health (NIH). This is a searchable science library which hosts articles from all around the world, in whatever language they were published in plus English. You can search any valid medical term — for instance, use the full name of your disease rather than its initials, for better results:
Here, you can see that I typed out “complex regional pain syndromes” instead of CRPS.
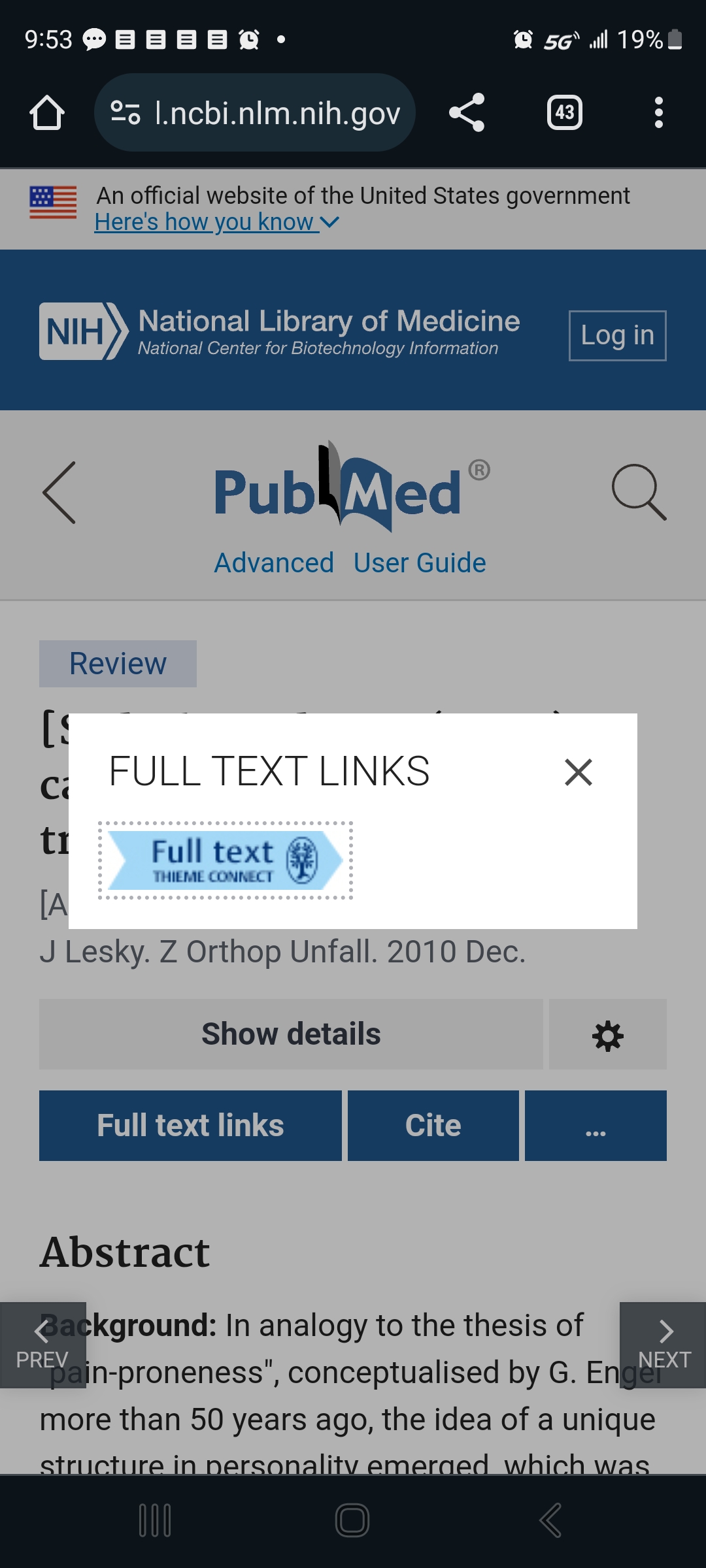
Some of them have full articles that are free to read (look for “Full Text Link”) …
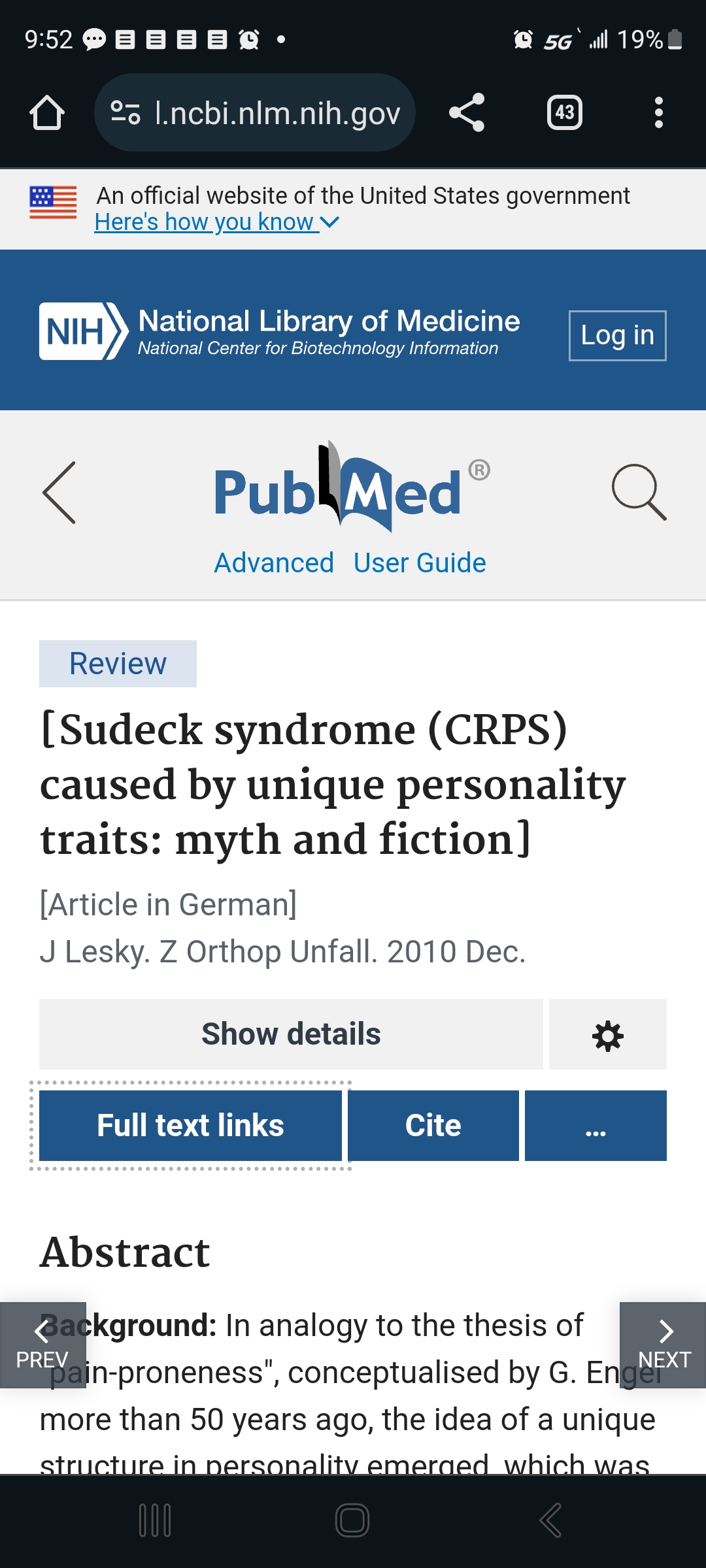
The square brackets around the title tell you it originated in another language. The note under the title tells you which one. Good science is done all over the world. I’m glad we can access so much of it!This image shows what pops up when you touch the Full Text Link button.This is the original site that published this paper. As you can see, it’s in German here, but an English translation is also printed below the German version. For better or worse, English is the world language for science and medicine. I feel lucky being born into an English-speaking family, because it’s tough to learn. All those synonyms… and the crazy spelling!
…But most will show only the abstract, that is, the high-level overview of what the study is about. For our purposes, that’s the most important thing, so it gives you something useful to work with.
The interface gives you options for saving, sending, and citing the articles.
Touch the “…” button to get this helpful menu. If you get a free account with the NLM, you can use these to help you keep your studies organized and accessible.
To use these, just touch or click the one you want. They do exactly what they say they will.
If you touch one of the menu options that requires them to store the info on their side — like “Collections”, “Bibiography”, or “Citation Manager”– it will give you what you need to sign in (if you already have an account) and, at the very bottom, the option to “Sign up”:
The site is very helpful; just slow down and let yourself look at one thing at a time.
Once you feel more self-assured, try out Google Scholar. It’s smaller in some fields and generally less selective, but that can be good. I suggest saving it for later only because it’s got fewer guard-rails. We’re all different, though, and you might find that easier.
These two libraries aren’t identical. They do overlap.
A word about MeSH terms
MeSH stands for Medical Subject Heading. It’s a curated list of specific terms used in the National Institutes of Health materials. This kind of consistency is necessary when organizing a stupendous medical database like the National Library of Medicine.
MeSH terms are listed at the bottom of each article. If that article was useful, you can click the MeSH terms to have them saved to your PubMed search history:
I’ve circled the heading “MeSH Terms”, where it appears below other back-matter after the article.
Here’s a tip: when using their Search tool, don’t worry about capitalization, but be very particular about spaces and punctuation. Copy them exactly.
Using MeSH terms will improve your future searches, because it makes the most of the databases self-referencing mechanisms.
Trust your eyebrows
Best tool in your mental toolbox: when you’re reading sentences you know you do understand and, yet, you feel your eyebrows moving around on your forehead… that logic is not right.
The scientist might be misinformed, biased, pulling a fast one, or just plain wrong, but it doesn’t really matter which — that logic is not right. The underlying pattern-matching part of your brain can tell. That’s a primitive part of the brain and, when you’re paying attention to it, it’s extremely hard to fool!
Trust your eyebrows. If you want to, save the article and come back to it when you know more, so you can figure out where the problem is. I assure you, there is one. Your eyebrows don’t lie.
Feed your brain
Reading science is hard work and brains are big hungry things at the best of times. Feeding it right can be a huge help.
Meds & caffeine
If you’ve got attention problems, adjust your meds and caffeine to give you some extra focus when you’re reading science. It’s a lot more fun that way!
Smart produce
Green, blue, and purple foods are absolutely marvelous for brains — and pain. They feed the nerves, literally. I know you needed an excuse to eat more blackberries, blueberries, collard greens, and rocket salad, aw shucks.
I also know it’s not the cheapest stuff in the market. Explore your local options for farmer’s markets, roadside stands, produce sales, and organized assistance like EBT/food stamps and healthy-living programs giving more access to produce in the state, like they have in Massachusetts and California and other places.
This is a great opportunity to learn more about your condition and to bring what you’ve learned into your life (more on that later), and the upfront effort pays off so much in the end.
Body-safe phenylalanine
Obviously, if you’re prone to phenylketonuria, skip this part! IYK,YK.
Also, keep in mind that this can have an effect on some meds — sometimes giving them a boost, sometimes making things worse. Be sensible, do your due diligence, and study it up for yourself if you’re interested. Also, use your self-documentation skills: note what you do and what it does to you, change what needs to change, and take responsibility for the results of your choices. We are our own best caregivers.
I’m discussing the physiological activity of this thing with the weird name, and what I’ve found in my life and those closest to me. This isn’t any kind of assurance that it’ll do good for anyone else. Put it no further than “hmm, maybe” in your mental filing system and do your own further research to validate what I say and get an idea how it might work for you, yourself.
Basically, phenylalanine is a precursor to the “up” side of the neurotransmitter suite, dopamine and norepinephrine and even epinephrine (they all transform into each other as needed). These neurotransmitters carry messages among the parts of the brain involved in learning and memory. Taking in phenylalanine can have a truly astonishing effect on attention and memory WHEN you’ve got fundamental deficits, as do people with central and longstanding pain and some other conditions.
TL;DR — If it doesn’t make an obvious difference in less than an hour, you don’t need it.
I’ve trialed using aspartame, which went well for me. (Discussing my results with my doctor paved the way to including SNRIs in my med regime, to my considerable benefit.)
Food sources of phenylalanine
This is where hard cheese and smoked or processed meat shine. They’re rich natural sources of phenylalanine. They also have saturated fats which, in moderate doses, seem to help with pain and brain symptoms.
As a moderate part of a well-balanced diet, folks.
This hasn’t been well-studied; it’s one of those things you pick up after being involved with self-managed patients for over 30 years.
It doesn’t take much. I found that 2 or 3 bites of aged cheddar would absolutely light up my brain for 45 min to an hour and a half, depending on my deficit.
One pal of mine keeps meat jerky sticks on hand for study sessions. Aged cheese works better for me; jerky works better for them.
Now, unfortunately, mast cell activation problems have moved cheese and smoked meat out of my diet. When I need a brain boost, and it feels like cheese might help, I have to use a supplement instead.
Supplementing phenylalanine
It’s more measurable to use a supplement called DLPA, or d,l phenylalanine. It’s a blend of natural and manufactured forms of phenylalanine. One works better for pain and another for depression, but the blend seems well-tolerated and helps both. Phenylalanine suppresses certain inflammatory kinases and may help suppress pain at the spinal root (that is, right where the base of the peripheral nerve path comes out of the spine) as well as helping with mentation and cognition. (Sarcastic Sister notes: The recent science about it magically disappeared in the wake of the “war on pain meds” and I won’t pretend to understand why.)
There is a maximum recommended dose before it gets toxic, but if you’re seriously thinking about that, you’ll want to do your own studying, and might want to talk to your doctor about SNRI meds as a possibility. (The N is for norepinephrine, which phenylalanine supports.)
Why bother with learning how to read science?
Knowledge and understanding are the most powerful tools you can have for dealing with complex chronic health problems. It may or may not change what you have to deal with, but it certainly gives you more and wiser options about how to deal with it.
Even if you aren’t ready to start now, you can circle back around to this whenever you want. It’s attainable; you can do it. It’ll always be there (although individual articles and topics may come and go.)
The patients who learn the most and put that to work in their own lives, are the patients who most consistently beat the odds and have the best quality of life over time.
Therefore, better information leads to better living with complex chronic illness. My HIV patients taught me that 32 years ago at my first nursing job, and it’s truer than ever now.
Note: Nobody here says it’s easy. That said, our complex chronically ill lives are never easy.
Pretending that getting through the day is not, itself, almost a superhuman task is a disservice to our strength, so let’s just start off by recognizing that everything we do is really hard work.
Knowing that, I have found that the effort of learning and applying what we learn pays off a whole lot more than passively waiting to be saved and feeling rotten all the while — and still being wrecked & exhausted.
I can whole-heartedly recommend learning and figuring things out. It’s a winner.