I headed to psychotherapy after texting, “I’m on my way. I’ll see you in person today, barring the unexpected”
I was feeling a bit cautious, because a couple hours before, the thought had come to me, “when things get hectic, trust your training.”
What training? Was I about to have a series of intrusive thoughts harking back to the times I’ve had to file restraining orders, one of which magically disappeared and I had to flee the area – right before Christmas? I hoped not. Martial arts training has certainly come in handy, but come on…
No, no intrusive thoughts, but I did wonder which set of training I should have in mind.
A few miles down the interstate, I saw a pickup truck stopped dead, and a sedan facing it.
People were only just getting out of the truck. I put my flashers on and pulled in behind.
I definitely trust my training in this kind of situation. I put my anxiety to one side and sailed in.
The only person to worry about was a littlie in the back of the sedan. Had spontaneous pulse – a good one – and respirations. He could speak, to the limit of saying, “I want my Mommy” (sound of heart-strings tearing), so I checked his spine at his neck. It was there, but not quite right. Once he could speak more, he told me his neck hurt where I touched it (I’d been holding his head & neck stable since I felt it). As I told the fire department medic later, “on me, it’d be a chiropractic adjustment. On a littlie that age, I’m not sure.” He nodded and sent his buddy in with a pediatric cervical collar.
Littlie’s mother was on the phone the whole time with him. So much love swirling around in that car. I told the Dad that I noticed it, and that it’s healing.
At each stage – or rather, just before the next round of excitement – I explained to Littlie that there would be more people, highly trained people who really cared about him being okay. Let him know roughly what to expect at each stage. Coached him to go along with things as well as he could. When the fireman asked him to squeeze his finger, he squeezed my hand instead (sound of heart melting).
I could see most of my words going over his head (as expected), but I could also see the sense of reason and structure calming his exhausted and shocky brain so he could tune in a little more.
I grew up in a musical household, so naturally I hummed pretty little made-up tunes and it visibly calmed him – and possibly his parents too, a little.
I’ve been working on learning how to stabilize a shocky system for 25 years, on top of my trauma nursing work. I’m only a patient – and a nerd – but still, I have lots of good training. I trusted my training in that, too.
I gave his mother my number right before the fire department and EMTs rolled up. I think it was a training day, because there were 7 or 8 more people there, one of them a cheerful charming know-it-all (every team needs one of those) who got the best responses out of Littlie.
I let the kid know I had to go but his Mommy would stay on the phone with him and he’d be cared for by these really nice people. Told his Mom I loved her kid and he was terrific (sound of heart-strings pulling).
Once his c-collar was on (definitely a training day; I helped get it positioned and sealed correctly in the end) and they had the gurney ready, I realized I had to stand up. After perching my crippled butt by one hip on a steel door frame for half an hour. In front of people. Specifically, a total of 9 or 10 fit, athletic slabs of beef (-cake) no less than 10 years younger than me, and most of them half my age.
This was not going to be great for the ego, but I knew I could get a laugh out of it.
So I used both arms and every available leg (which was slightly less than 2) to lever myself upward, saying, “I’m an *oooold* trauma nurse” by way of cover, and squirmed through the kindly, protective testosteronic press and into fresh air.
I signed off with everybody and retreated to my comfy car.
I called my psychotherapist and said, “Remember what I said about ‘barring the unexpected?’…”
We had a phone session once I was safely off on a side street and in a proper parking space. She was full of commentary about how I applied those psych skills and met psychosocial and informational needs appropriately, as well as the nursey stuff. So yeah, that was good…
… because my brain was churning constantly about every single moment and thought and decision for an entire hour. Looking for a fault. Looking for something I’d missed or where my training had lapsed or been forgotten. Cycling through, over and over, looking for any lapse.
This used to be how I improved my skills – look for errors, even tiny ones, and figure out how to prevent or avoid them in future. Now, it’s just my ADHD brain torturing me.
And computer says Nope. Failed to suck. I’m pretty sure I failed to suck. That’s a relief.
I’ve been thinking about it pretty much nonstop, but rather than worrying myself woolly, I got an organizing thing for my car and picked up some food. Both of these are calming, grounding things, perfect for pulling my adrenaline out of the stratosphere.
Then I crawled home and had fresh corn and gluten-free carrot cake for dinner. It’s good to have a little sweetness when your body is still convinced the world is full of excoriation.
I’ve had no calls from them and I don’t expect one. They’ve got to be absolutely wrung out regardless of how things went. The kid comes first, and then comes their own care and self-management.
They don’t have to think of me ever again: I know how shocking and painful it could be to revisit the moment.
I’d love to know. I hope like crazy that the kid came out of it OK. I never got to follow up with patients when I was a nurse (because confidentiality), and I’d sure appreciate it if this family wanted to give me a heads-up just to soothe that old itch.
All that being said, I want all you non-nurses to know that they don’t owe me one word of contact or one moment of concern. I was in the right place at the right time with the right training, and I trusted my training. That’s what we do.
They have the hard part: figuring out next steps with a shook-up and possibly injured Littlie who was going home early because he was already ill.
That kid was having a rotten day.
I sure hope it got better.
Forestalling future problems
I don’t have a jump-kit for my car. That could be a problem in the future. I was lucky this time because all I needed was my brain, arms, hands, and voice.
It’s probably the 6th or 7th accident I’ve stopped at and I really do know what’s needed at the roadside – and it isn’t much. I used to get confused by the fact that I didn’t have a stethoscope, oxygen on tap, i.v. gear, and All Tha Meds. Once I’m on scene, though, it gets very easy.
Any blood or, indeed, anything wet? Nitrile gloves, packed up in pairs and stowed in a closed outer pocket to keep them clean & dry and easy to get on.
Heaven forbid, does anybody need CPR? This very rarely happens, but when it does, I don’t want to have to dig for the needful. I physically can’t do chest compressions (though I can coach any able-bodied person properly) but I can darned well use a mask with a one-way valve as if I’ve had years of practice. Years. You don’t have to have that (the training has shifted away from doing rescue breathing) but I feel that I do.
Pressure dressing? Kerlix. Sling? Kerlix. Wound cleaning? Kerlix makes a great sponge. Wound wrap? Kerlix. Piece of clean water-resistant paper to slap over a bubbling wound? Wrapping off a Kerlix.
So, plenty of Kerlix.
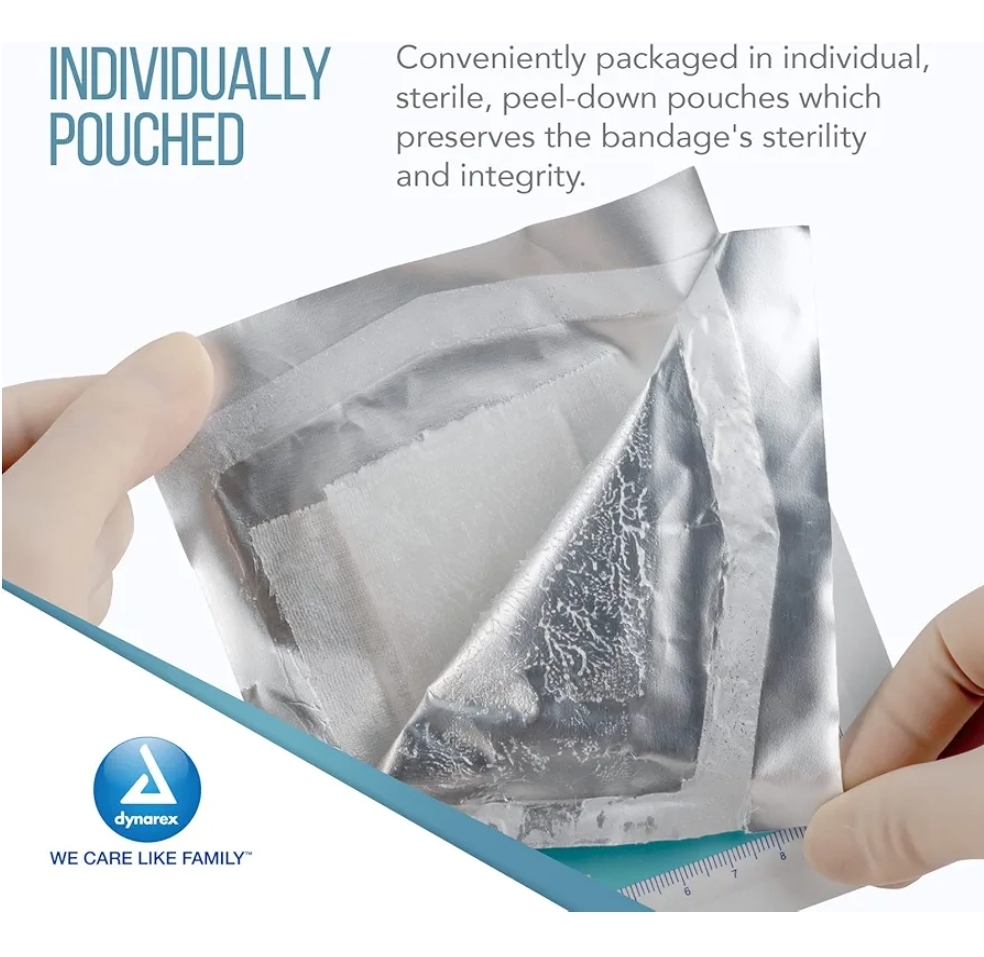
Road rash? Plenty of saline rinse (and a Kerlix) then a petroleum dressing to stabilize the damage until the ER can do a better job.
And possibly most essential: disinfectant cleansing towels, individually wrapped and big enough to grab. Those get used before if there’s time, during if the patient wants cleaning up, and definitely afterwards.
Because allergies & neurological reactivity, I stick with ethyl alcohol 70%.
Secure the mess. A gallon-sized zip bag or 2 for garbage and wrappings. Having a garbage bag is one of the things that separates rescuers from ego-trippers.
Oh, did I say that out loud? Sorry. I don’t want anyone not to stop & help… I just wish that, if they’re going to the effort of bringing gear, they could pick up a bit. Seeing blood and mess is not good for survivors & passers-by.
I got all these online for about $10 each, and also got a clear bag (with outside pockets) to put the kit in.
I’ll keep backstock at home.
What I don’t carry
Blood pressure readings, stethoscopes, and pulse oximetry are at-home and in-hospital concerns: we want to know if what we’re doing is working over time and refine our understanding of the body’sfunctional state.
In the field, the main issue is not whether the patient has rales or a murmur, but whether the lungs and heart are keeping them alive – a much simpler, larger-grained issue.
So, these tools might be nice to have, but for a noodle-noggin like me, they’re an added complication and a bunch of expensive equipment to lose at the scene.
In the field,
You need to keep pulse and respirations going,
the spine stable,
make sure the inside stuff stays inside
and in place,
and (as much as possible) the outside stuff stays out – or at least doesn’t move much where it’s inside the person.
And that, ladies and gentlebeings, is Advanced First Aid and Basic Life Support in a nutshell. You’re welcome 😊 Now go get that training… please?
I wrote the start of this for a fellow spoonie today and realized it’s a good starting point for a subject most people find overwhelming: reading medical science when you’re starting off as a non-scientist.
The article I cite first is a good example to start with, because it’s written well and has passages of clear English to work with. So…
I suggest reading the abstract and introduction. After that, just skim the first sentence of each paragraph, since (in science writing) that tells you what the paragraph is about.
If the first sentence makes no sense, skip that paragraph.
If you can figure out the first sentence, glance at the rest of the paragraph to see if there’s any more to glean. If not, move on..
It’s a skill
Reading science is a skill, and skills take time to master. That’s expected! Share what you glean with your doctor and ask them to help you understand it better.
Honestly — this isn’t to puff myself up, it’s just the nature of patients to dis themselves, so hear me out — if you can read my stuff and make out half of it, you are plenty smart and literate enough to start reading science. It’s just work and time, and the time will pass whatever we do, and the work will get easier with time. We just have to take care of ourselves and pick our time, when we’re chronically ill.
Using the right amount of honey
Doctors might give you attitude about comparing your Google search to their medical degree, but that’s not what you’re doing: you’re studying up on your condition, which is wise, and you’re expanding your info base on this thing that has imposed on your life, which is survival.
So, feel free to correct them sweetly, and don’t be afraid to pour some admiration on them if it helps them to re-focus on your information-gap.
The point is not who knows more overall. That’s not in question. When you talk to your doctor, you’re talking to someone who had to memorize, for instance, the Krebs cycle (here’s a partial explanation: https://www.medschoolcoach.com/the-krebs-cycle-mcat-biochemistry/) — so, yes, they have a depth and nuance of knowledge that’s nearly impossible to replicate without going to medical school.
They like having that acknowledged, because they take a lot of painful flak for not knowing everything about everybody’s illnesses all the time, and they need to know that you know what an effort they made to be able to work as a doctor.
So, it’s good to acknowledge that enormous effort.
Then they are usually able to hear you when you clarify that you’re not arguing with them, you’re trying to improve your understanding of this thing that affects you so profoundly. You trust them to help because of their knowledge.
Trust. Help. Knowledge.
These are keywords because they are core professional values for most doctors.
They’re important to acknowledge, and great to invoke and rely on.
That said… if you can’t rely on these characteristics in your doctor, even after you tell them that that’s what you need, then it might be time to find another doctor if you can. These core values are far more important than whether a doctor has good social skills or a good handshake.
When all is said and done, guess who has to live (or not) with the outcomes? It’s you. While the doctor is the subject-matter expert on the medical info around your condition, you are the subject-matter expert on being in your body and dealing with the fallout. There’s a degree of respect that should go both ways, though modern practice makes that hard.
The key to reading science is realizing — or at least, going ahead as if — you’re perfectly capable, and just need to practice. Science is written by humans, and you’re a human too.
1. You are a perfectly sensible person. If you’re reading this, you know how to read (or access translations from) English; also, you have access to a whole world of dictionaries. MedlinePlus is especially helpful in explaining concepts and helping us learn to read medical stuff.
2. Not all scientists can write well in English, and none of them write in English all the time. That’s okay. They went to school for a long time to get extra vocabulary and learn to do what they do; good for them. They’re still people, and they have to write in English at least some of the time. That’s where you can come in.
3. You can read the English just fine. Trust yourself and take time. With practice, you can learn more lingo over time, and get better at reading more science.
Just work from what you can understand now, and let that grow over time. You’ve got this.
Choosing credible sources
While you’re learning to read science, start where you can and work from there. As you get more confident and your understanding grows, you’ll learn to be choosier.
The gold standard for science info
When learning how to assess science, you’ll hear a lot about placebo-controlled, double-blind studies and that method is often important. This method of science gives us more reliable statistical probabilities about whether something will work in a certain situation. The statistical probabilities become reliable when several thousand people (“subjects”) have been tested, probably over many different studies.
With rare diseases, this is obviously pretty unlikely, so we have to work with less scientific certainty. C’est la vie.
Statistical probabilities have more limited value for patients than doctors, because we’re individuals, not pooled data. There used to be a phrase used in medical school: “Statistics mean nothing in the case of the individual.” This has gone by the wayside a bit, but it’s still true.
We may have to cast our nets further afield, because we’re looking for clues that might help us, personally. Be aware when you’re doing that, and put those science reports in your mental “hmm, maybe” folder.
I showed a case study that had a marvelous impact to one of my best doctors. He said to me, “If I could put that effect in a bottle, I would. It worked for that person, and we have no idea why. We do know that it doesn’t work for all these other people. Everybody’s different. Figuring out how to apply one thing to help a lot of people is our holy grail!” Lloyd Saberski, MD.
And that’s why doctors rely on the pooled data gathered from the scientific method. They want to help as many people as possible with each thing they try. Otherwise they fear they’ll spend too much time chasing rainbows.
We patients have to find our own rainbows, just as we have to count on our doctors to keep an eye on what’s statistically worth trying. It really is teamwork, and we both need to do our jobs.
What’s peer review?
Before you give a study to your doctor, it’s worth checking if it’s from a peer-reviewed journal. Don’t expect them to put too much stock in it otherwise.
Peer review means that other people in related fields have checked it over for sanity and validity. This is important for us patients, as well as the doctors who rely on the information.
You can Google whether the journal your article was first published in is a peer-reviewed journal. JAMA, BMJ, and the Lancet are all reliably peer-reviewed.
The value of literature reviews
Then, after a fair amount of studies have been done on a topic, there’s usually a literature review. This is when a qualified scientist takes a close look at all the studies, throws out the ones that were badly designed or poorly run (because bad technique creates bad data. “Garbage in, garbage out”) and writes an overview of what the current good science says.
They also discuss the strengths and weaknesses in the data, and suggest where future science funding could go, in light of the science so far.
Literature reviews are wonderful places to improve your knowledge of your disease/condition, expand your vocabulary, and get a lot better at understanding what goes into the science on your condition in the first place.
For instance, it used to be widely believed that most people with Complex Regional Pain Syndrome had had traumatic childhoods. (“Blame the parents” LOL.) There was a literature review done on about 30 years’ worth of studies, and it turned out that almost all of them were so badly-designed, poorly run, and calculated with so much bias, that nearly all of the studies had to be thrown out!
This taught me very important lessons:
– Just because most people say it, doesn’t mean it’s right, even if they should know better. This is an excellent attitude to have while reading science.
– Methods matter. You’ll learn over time how to sense whether the methods used are appropriate to the topic studied. The wrong method can lead to truly bogus results. The method has to fit the material.
– People lose their minds when they think about pain, as well as when they think about childhood trauma. In practical terms, this means I have to approach all normal (non-CRPS) people’s reasoning about my condition (which is characterized by relentless agony which a non-CRPS’d brain cannot even conceive of) with compassionate criticism. They do not know what it’s like, nor how to live with that pain and still think rationally. They’re not able to know. I don’t want them in a position where they do know, because that’ll mean their lives are as battered as mine is.
Therefore, every word they say has to be filtered through my awareness of how their minds get lit up by unreason, when they think about my pain. This, believe it or not, is perfectly natural. (Look up “amygdala hijack” for background on this mechanism.)
I survive because I’ve learned to substantially displace or ignore one of the most powerful primitive signals in the human body. That isn’t natural, and nor should it be.
These scientists mean well, without question. However, their logic is necessarily fractured when thinking about this, because they lack my tools for facing it. I need to dig into their data and methods before I can buy into their conclusions.
That’s good to know!
The conclusion of that literature review? CRPSers are likely (not guaranteed) to have had relatively eventful lives. Whether the events were traumatic or wonderful wasn’t relevant to our probability of developing CRPS.
In other words, we live in interesting times!
Where to find science to read
Google pubmed, and you’ll find the National Library of Medicine (NLM) division of the National Institutes of Health (NIH). This is a searchable science library which hosts articles from all around the world, in whatever language they were published in plus English. You can search any valid medical term — for instance, use the full name of your disease rather than its initials, for better results:
Here, you can see that I typed out “complex regional pain syndromes” instead of CRPS.
Some of them have full articles that are free to read (look for “Full Text Link”) …
The square brackets around the title tell you it originated in another language. The note under the title tells you which one. Good science is done all over the world. I’m glad we can access so much of it!This image shows what pops up when you touch the Full Text Link button.This is the original site that published this paper. As you can see, it’s in German here, but an English translation is also printed below the German version. For better or worse, English is the world language for science and medicine. I feel lucky being born into an English-speaking family, because it’s tough to learn. All those synonyms… and the crazy spelling!
…But most will show only the abstract, that is, the high-level overview of what the study is about. For our purposes, that’s the most important thing, so it gives you something useful to work with.
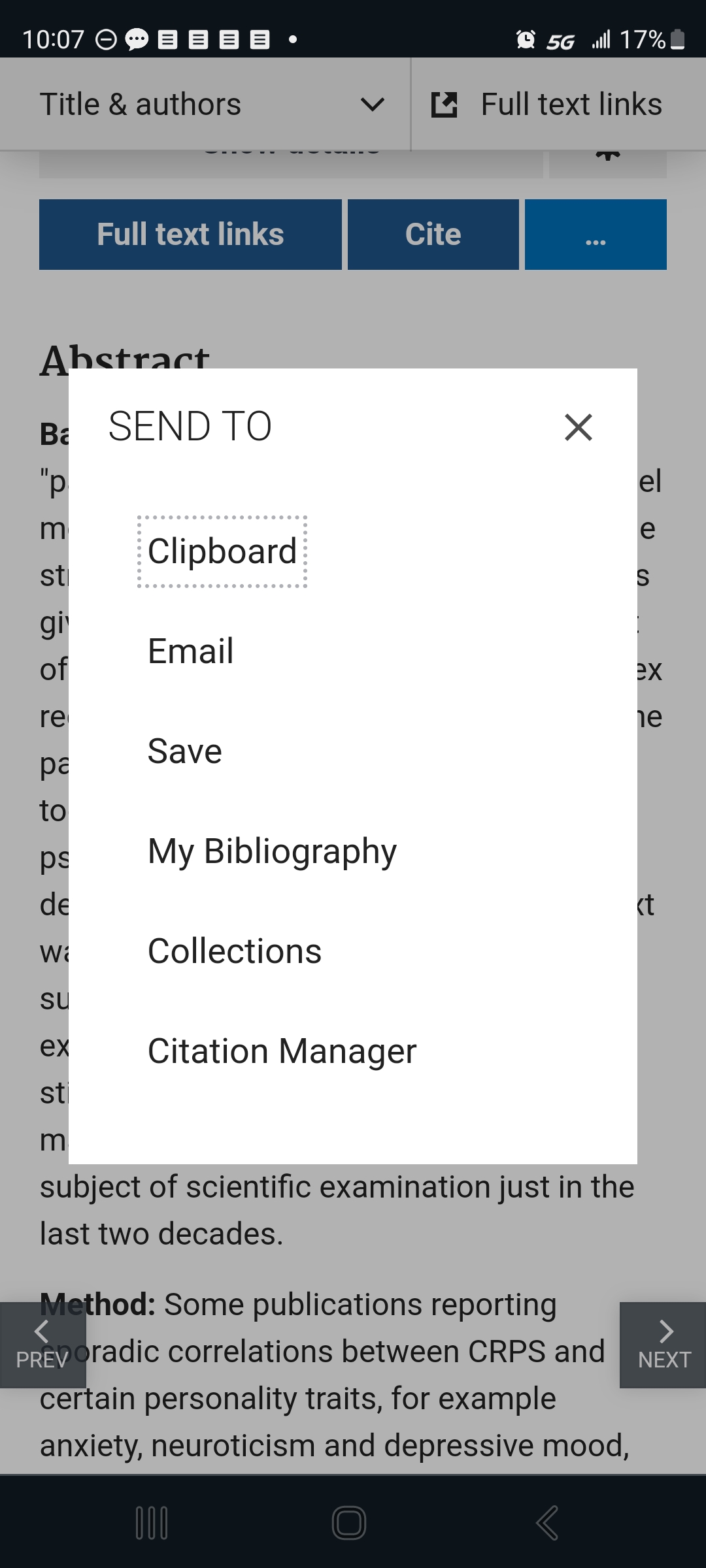
The interface gives you options for saving, sending, and citing the articles.
Touch the “…” button to get this helpful menu. If you get a free account with the NLM, you can use these to help you keep your studies organized and accessible.
To use these, just touch or click the one you want. They do exactly what they say they will.
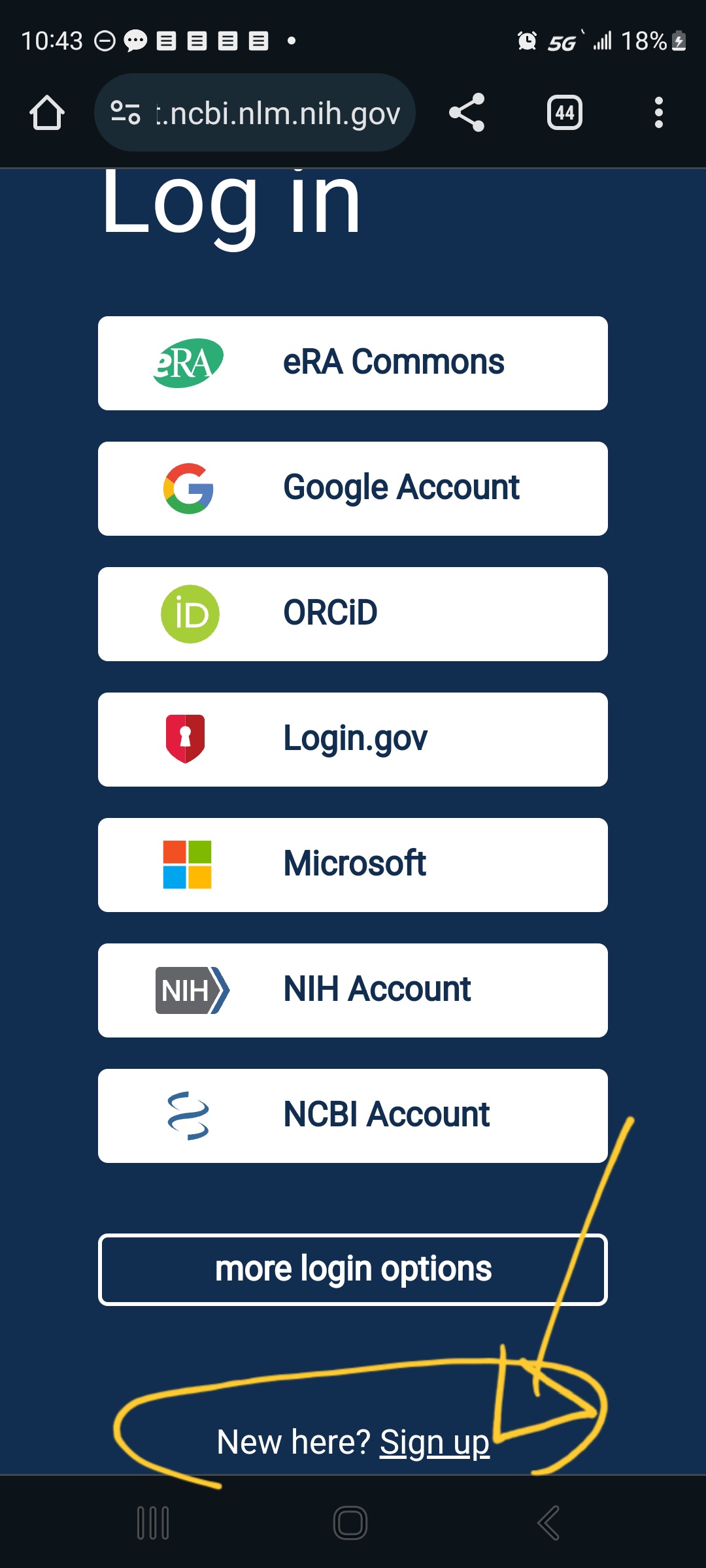
If you touch one of the menu options that requires them to store the info on their side — like “Collections”, “Bibiography”, or “Citation Manager”– it will give you what you need to sign in (if you already have an account) and, at the very bottom, the option to “Sign up”:
The site is very helpful; just slow down and let yourself look at one thing at a time.
Once you feel more self-assured, try out Google Scholar. It’s smaller in some fields and generally less selective, but that can be good. I suggest saving it for later only because it’s got fewer guard-rails. We’re all different, though, and you might find that easier.
These two libraries aren’t identical. They do overlap.
A word about MeSH terms
MeSH stands for Medical Subject Heading. It’s a curated list of specific terms used in the National Institutes of Health materials. This kind of consistency is necessary when organizing a stupendous medical database like the National Library of Medicine.
MeSH terms are listed at the bottom of each article. If that article was useful, you can click the MeSH terms to have them saved to your PubMed search history:
I’ve circled the heading “MeSH Terms”, where it appears below other back-matter after the article.
Here’s a tip: when using their Search tool, don’t worry about capitalization, but be very particular about spaces and punctuation. Copy them exactly.
Using MeSH terms will improve your future searches, because it makes the most of the databases self-referencing mechanisms.
Trust your eyebrows
Best tool in your mental toolbox: when you’re reading sentences you know you do understand and, yet, you feel your eyebrows moving around on your forehead… that logic is not right.
The scientist might be misinformed, biased, pulling a fast one, or just plain wrong, but it doesn’t really matter which — that logic is not right. The underlying pattern-matching part of your brain can tell. That’s a primitive part of the brain and, when you’re paying attention to it, it’s extremely hard to fool!
Trust your eyebrows. If you want to, save the article and come back to it when you know more, so you can figure out where the problem is. I assure you, there is one. Your eyebrows don’t lie.
Feed your brain
Reading science is hard work and brains are big hungry things at the best of times. Feeding it right can be a huge help.
Meds & caffeine
If you’ve got attention problems, adjust your meds and caffeine to give you some extra focus when you’re reading science. It’s a lot more fun that way!
Smart produce
Green, blue, and purple foods are absolutely marvelous for brains — and pain. They feed the nerves, literally. I know you needed an excuse to eat more blackberries, blueberries, collard greens, and rocket salad, aw shucks.
I also know it’s not the cheapest stuff in the market. Explore your local options for farmer’s markets, roadside stands, produce sales, and organized assistance like EBT/food stamps and healthy-living programs giving more access to produce in the state, like they have in Massachusetts and California and other places.
This is a great opportunity to learn more about your condition and to bring what you’ve learned into your life (more on that later), and the upfront effort pays off so much in the end.
Body-safe phenylalanine
Obviously, if you’re prone to phenylketonuria, skip this part! IYK,YK.
Also, keep in mind that this can have an effect on some meds — sometimes giving them a boost, sometimes making things worse. Be sensible, do your due diligence, and study it up for yourself if you’re interested. Also, use your self-documentation skills: note what you do and what it does to you, change what needs to change, and take responsibility for the results of your choices. We are our own best caregivers.
I’m discussing the physiological activity of this thing with the weird name, and what I’ve found in my life and those closest to me. This isn’t any kind of assurance that it’ll do good for anyone else. Put it no further than “hmm, maybe” in your mental filing system and do your own further research to validate what I say and get an idea how it might work for you, yourself.
Basically, phenylalanine is a precursor to the “up” side of the neurotransmitter suite, dopamine and norepinephrine and even epinephrine (they all transform into each other as needed). These neurotransmitters carry messages among the parts of the brain involved in learning and memory. Taking in phenylalanine can have a truly astonishing effect on attention and memory WHEN you’ve got fundamental deficits, as do people with central and longstanding pain and some other conditions.
TL;DR — If it doesn’t make an obvious difference in less than an hour, you don’t need it.
I’ve trialed using aspartame, which went well for me. (Discussing my results with my doctor paved the way to including SNRIs in my med regime, to my considerable benefit.)
Food sources of phenylalanine
This is where hard cheese and smoked or processed meat shine. They’re rich natural sources of phenylalanine. They also have saturated fats which, in moderate doses, seem to help with pain and brain symptoms.
As a moderate part of a well-balanced diet, folks.
This hasn’t been well-studied; it’s one of those things you pick up after being involved with self-managed patients for over 30 years.
It doesn’t take much. I found that 2 or 3 bites of aged cheddar would absolutely light up my brain for 45 min to an hour and a half, depending on my deficit.
One pal of mine keeps meat jerky sticks on hand for study sessions. Aged cheese works better for me; jerky works better for them.
Now, unfortunately, mast cell activation problems have moved cheese and smoked meat out of my diet. When I need a brain boost, and it feels like cheese might help, I have to use a supplement instead.
Supplementing phenylalanine
It’s more measurable to use a supplement called DLPA, or d,l phenylalanine. It’s a blend of natural and manufactured forms of phenylalanine. One works better for pain and another for depression, but the blend seems well-tolerated and helps both. Phenylalanine suppresses certain inflammatory kinases and may help suppress pain at the spinal root (that is, right where the base of the peripheral nerve path comes out of the spine) as well as helping with mentation and cognition. (Sarcastic Sister notes: The recent science about it magically disappeared in the wake of the “war on pain meds” and I won’t pretend to understand why.)
There is a maximum recommended dose before it gets toxic, but if you’re seriously thinking about that, you’ll want to do your own studying, and might want to talk to your doctor about SNRI meds as a possibility. (The N is for norepinephrine, which phenylalanine supports.)
Why bother with learning how to read science?
Knowledge and understanding are the most powerful tools you can have for dealing with complex chronic health problems. It may or may not change what you have to deal with, but it certainly gives you more and wiser options about how to deal with it.
Even if you aren’t ready to start now, you can circle back around to this whenever you want. It’s attainable; you can do it. It’ll always be there (although individual articles and topics may come and go.)
The patients who learn the most and put that to work in their own lives, are the patients who most consistently beat the odds and have the best quality of life over time.
Therefore, better information leads to better living with complex chronic illness. My HIV patients taught me that 32 years ago at my first nursing job, and it’s truer than ever now.
Note: Nobody here says it’s easy. That said, our complex chronically ill lives are never easy.
Pretending that getting through the day is not, itself, almost a superhuman task is a disservice to our strength, so let’s just start off by recognizing that everything we do is really hard work.
Knowing that, I have found that the effort of learning and applying what we learn pays off a whole lot more than passively waiting to be saved and feeling rotten all the while — and still being wrecked & exhausted.
I can whole-heartedly recommend learning and figuring things out. It’s a winner.
My poor ol’ body has been carrying an unfair load for a long time. It does its very best, but the dice are loaded and, of course, aging intensifies all the problems and reduces all the healing mechanisms that keep it going.
Its experience as a physio-electro-mechanical system constantly in search of homeostasis – that is, a flexibly stable state — is seriously affected by the fact that it’s got these conditions which seem to think that homeostasis is a nice big target to shoot at and instability is fun. Woohoo!
I’m having what I suspect is a barrage of endocrine stuff which, among other things, makes my body’s pain and ability to adapt simply go phut.
CW: graphic descriptions of pain.
The bone pain triggered by walking is off the charts. Now I get one walk per week, it has to be less than 2 miles, I come home and go straight to sleep for 3-4 hours after, and have no attention or stamina the following day; I have to write off that time completely. My muscles and tendons feel like they’re filled with burning shards of glass. My leg bones feel like gelid columns of fire, like stiffened napalm, so that I’m half-afraid they’ll go squish and disintegrate under me, and who knows where that napalm would go if they did.
Honestly, that’s weird.
Activity is good. Moving is the secret of life.
Used to be.
My cycles still help at times. The recumbent trike, while it unloads my lower back beautifully, exacerbates my neck posture, which redounds into headaches for days. It also takes up a huge amount of space (it’s over a meter wide), so I have to stick to the wider paths and not try to use it in winter. However, it gave me back a lot of life last summer and fall. I had no idea what this year had in store for me, or honestly I’d have gotten something cheaper. Less safe, less comfortable (despite the neck thing), less of a joy to ride, because that trike is fantastic of its kind and fits like a glove… below the neck.
The cute retro bicycle? I didn’t sell it (though I probably should). I’ve been able to use it on some good days, but unfortunately I was still right about the road vibration on my spine and arms, and the pressure on my carpal tunnels. But it does fit into narrower spaces.
So, at this point, I have 3 modes of transport which used to work well, but this absolutely relentless business of being chronically ill has nearly, if not quite, taken them away.
Breathe, me. It’s just a problem.
It’s just a problem, and problems are meant to be solved.
I have a rowing machine which is currently my safest option for activity, although it doesn’t get me anywhere. It uses most of the body’s muscles, and I can tell because I can go for 6-8 minutes before I get sick and light-headed and the burning shards turn up. I’ve been trying to go up from 6 minutes without making myself sick, but my body can’t get past the 7.5-minute barrier without the spiculated pain all over and the desperate exhaustion for days. And yes, I incremented very slowly, but it just won’t work.
Weird. I cannot get used to that.
Time was I’d row for 20 minutes at “fit man” level, and go even longer in the water. I wanted to get a sea kayak and use it for transportation; I loved the motion of kayaking and could not imagine a better way to start or end the day. Middle-distance running (3 to 13 miles, depending on how much time I had) was a lot more affordable and accessible, so I did that instead. I was one of those annoying people who really enjoyed running.
I try not to think about that. These kinds of losses are about so much more than “hey, I could do this thing, yay me”; it’s more about how I fit into life and engaged with the world around me, about the tools I had available to help me through the hard times and illuminate the good ones. So much is out of reach.
That’s life.
Breathe, me.
I’ve got more specialist appointments crammed into the next few months than I’ve had in years; possibly ever. The science is a lot further along than it was when I was working as a nurse, thank goodness. The reason why I get heavier when I don’t eat enough is technically understood. The trouble lies in getting people to believe it and trust that I’m telling the truth.
It’s very weird to me to be disbelieved: I’m white, well-educated, have big blue honest eyes, and present info well. Now, as a fat middle-aged woman, apparently I’m inherently much less credible. Obviously, I must be kidding myself (if only!) and comfort eating (if only!) and clearly just being too lazy to work out (if only!)
I have no idea how that works, because you don’t get to middle age with significant illnesses by being stupid or incapable of self-care.
Breathe.
Keep breathing.
Problems are meant to be solved.
I’ve been thinking over solutions to the “how to be able to get things done outside the house” issue. I have partial solutions – all of them depending on others or on problematic systems.
For now, they’ll have to do. I’m glad I’ve got even them, of course. For all the towering cost of agony, uncertainty, and logistics, it beats having none.
Keep breathing.
I have a good home that I love. That’s one huge thing right, an unbearably difficult problem that has definitely been solved. From here, I’ll just have to figure out the rest.
Up until I got the injuries that precipitated CRPS, I used to run about 3.8 miles (about 6.1 km) up and down a redwood canyon most mornings. It was a highlight of the day: watching the light stain the tops of those glorious trees, waking the birds as it went, until the whole forest was filled with the noise of thousands of adorable featherbrains screaming their fool heads off, and the spiraling redwoods were soaked in molten gold.
I sprained my ankles a few times, leaving them with permanent puffy-pads. One time it was a bad sprain (I was pretty sure it was broken, given the huge swelling and rapid bruising) and I had to crawl and hop the last mile-and-a-bit, but I got there in the end because I’m just that kind of bonehead. I drove my stick-shift to the ER because, after all, the foot was still attached and all I had to do was push a little.
…Bonehead. (With, admittedly, an unusually high pain tolerance.)
Got poison oak a few times, until I went back to using poison-oak honey in my tea for the passive immunity.
I was kind of a sucker for a challenge, and I liked figuring things out.
I also liked the boards they had laid across a sandy furlong of the path to keep the sand from getting ploughed too far by the horses. The boards were just tall enough to make me hop them, and I liked pretending I was a horse trotting through a series of in-and-outs as I popped over them one after the other.
Great way to start the day.
And then what happened?
The repetitive stress injuries of long hours with keyboard and mouse, led to a series of wrist surgeries and complications in a couple of years. The CRPS diagnosis took longer.
What with all the roots and stones and the sun being in my eyes for the latter part of the run, I did stumble a lot. Having to catch myself went from being a diversion, to a nuisance, and rather suddenly to a terrifying possibility with crippling results. I dared not land on my wrists, because that could be the end of my career and my ability to support myself.
After recovering from surgery, cardiovascular exercise just caused too much swelling and inflammation — for years. I found that counterintuitive, which means illogical and, for me, extremely frustrating.
Fast forward 24 years
And now, it’s now. The ongoing heat wave (and flash floods) are making my usual afternoon walks impossible. My body refuses to stay vertical when the temp is a stunningly humid 84 degrees F (28.8 C). This body-system and wet-bulb temps just don’t get along.
Meanwhile, my thyroid supplement is starting to take hold. This means that, while I’m not up to normal energy by a long way, I crave exercise like a junkie with healthy tastes.
The only time I can be outside is before 8 am.
It usually takes me until then just to get out of bed, because of dysautonomia.
It’s hard to describe the sensation of challenging your dysautonomia, but if you turn on a powerful electric milk-frother and throw that down your stomach, while putting your head inside a vice and trying to breathe through a sodden sock, as flesh-eating termites devour your limbs… well, you still won’t know what it feels like, but you’ll at least be in the right ballpark.
I have an agreement with my body where it will let me get up early for Really Important Things, like fasting lab draws and airplane trips; I just have to pay for it the rest of the day.
I decided that it’s time to move exercise back into that category and hope it adapts appropriately. This is going to be rough, but the skills I’ve learned might make it work.
The skills
First thing is, No Surprises. I think about getting up and out early, as I’m getting ready for bed the night before. I think about the early hush and the freshness of morning air. I wonder what birds I’ll hear. I look forward to it sincerely.
Next thing is, Lower Barriers & Eliminate Excuses. Water is at my bedside and clothes & shoes get picked out the night before. I don’t want to have to think about doing it, I just want to grease the slide out the door.
Third thing is, Wake And Ground Deliberately. Once my eyes are willing to open, I drink at least half my pint of water and then organize my spine (a series of moves and physical therapy stretches that make my spine feel properly engaged), and then get all the way inside my skin (tapping down the top of my left arm, up the bottom of the left arm, down my side and front, down the front of my left leg, grab my foot until I can really feel it top and bottom, tap up the back of my leg, over my kiester and up my back and side; then, do exactly the same thing on my right side; then, tap up my neck — tapping on alternate sides — and use my fingertips over my face; rub through my scalp to get all the scalp muscles awake and ready to encase my skull today; and nice big sigh to turn over the air in my lungs.)
It sounds rough for CRPS, but I’ve been doing this for a long time and my brain knows what to expect. That’s important.
It also works to apply pain cream instead of tapping. It’s fine to skip over bits that don’t let you touch them. It’s fine to use a very soft touch, or stroke with something soft like a bit of plushy fabric or a feather.
It’s about input for the skin that helps the brain remember and rehearse where your body is in space. This is an important tool for pushing back on CRPS. It literally recaptures parts of your brain that have been turned into pain-sensation, and makes them remember how to do body-sensation instead. Worth pursuing and persisting with.
After this, I check in and, if body says it’s willing to try, I swing my feet onto the floor. I finish my water there, sitting on my bed.
I Check In as I Sit Up, nicely hydrated and with no surprises. If all is well, I get up and check in with my legs. If they’re OK holding me up and flexing, then I climb into clothes and shoes, and head out for my walk.
I planned my walk the night before (“no surprises” really helps the autonomic system to cope!) so there’s nothing to figure out as I grab my phone and keys and head out.
I adjust the distance I’ll go depending on how I feel when Im out. Today, I got wildly nauseous when I was about at half my intended distance. Vomiting tears open my saggital seam, that tough band that forms the middle crease in a 6-pack. (I vomit very hard.) So, I sat down and smoothed down the texture of my thoughts until the nausea passed.
Then I did some t’ai chi and qi gong, focusing on moves that stabilize the autonomic nervous system and ending with a “microcosmic orbit” series I always enjoy. (Let me know if you’d like video of any of that.)
Once my internal system was going better, I bowed out and returned, snapping pretty pictures on the way.
Summary & Conclusions
I’ve gone about the same distance both days, though yesterday’s walk took less time — I didn’t have to sit down. Today’s walk was more up & down. I think I’ll stay on level ground the rest of this week and see how that goes.
I’m now fighting the urge to go to sleep. I fell asleep at 8:30 am yesterday, after getting in from my walk, and slept until 1:30 pm. Waste of a day, IMHO.
Maintaining a diurnal cycle (regular sleep/wake and eating times) is very important for taking care of yourself with dysautonomia. So, now that my thyroid is not completely in the toilet, I’m going back to fighting to keep hold of the day. I want some life back.
To be perfectly frank, I’ve spent most of the last 9 or 10 months just waiting for each day to pass in the hope that another day will be better, and if not, at least I’ll be closer to the right treatment.
Enough is enough.
It’s hard work, but so is life: I’m starting to take back my days. That starts with regular activity, because nothing re-regulates a dysregulated system like regular activity.
In the spirit of this blog’s brief as a “user manual for complex chronic spoonies”, here’s a health update after another interesting year (my personal year starts in May!) with notes on medical support & the relevant self-care for each problem area.
Cultural note:
In American slang, “the Back 40” was (is) probably the least obvious & accessible parcel of a farmer’s land. Either a lot of work or no work happened there, it was hard to find the person doing it, and the effort didn’t show until afterwards.
Good metaphor!
Areas of life…
Mom (& TL;DR): 2+/3, it kinda sucks but I’m getting doctors involved and they’re good. Adjust expectations downward a bit, because this could take awhile to resolve.
Endocrinology
I got a med with a toxic-to-me ingredient (maltodextrin; it’s specifically inappropriate for people with low thyroid!) and that set me back in inflammation, pain, mood, and thyroid function. That’ll take some time to recover from, but…
=> I’m doing All The Things, mostly hydrating & waiting & antioxidants.
Plus a thyroid med I tolerate well.
Not having thyroid supplementation at all for 4 days (after 2.5 weeks of thyroid with toxic crap in it) set my thyroid recovery back further, but let my mood come back closer to baseline and gave me more access to memory & coping skills.
=>More waiting, plus vitamin A, licorice root, and Maine seaweed for the iodine.
And lots of sleeping.
Dr:
I have an appointment with a good endocrinologist in June, which gives me time to look up his articles & see how he thinks, while brushing up on my endocrinology. (Being a passive patient doesn’t work well for me. Too much complexity & too little margin for error. I hope he can cope with a collegially-minded patient.)
G.I.
I tried heirloom corn flour, because I love masa and grits, and the industrial kinds of corn are too hard on me. (Pain, mood disruption, bit more brain fog.)
Well, it took longer than regular commercial corn, and it took making it a staple & eating it a couple times a day, but it turns out that organic heirloom corn can still do that to me. So, more waiting & more hydration, but after Day 2 of No Corn I’m already a little better. Yay!
Good news is, I’ve consistently been able to eat *enough* overall that my body’s starvation response is calming down! I’m no longer gaining weight daily (which is what my body does when it’s starving). I’m able to fit into my biggest clothes that *aren’t* stretchy, another yay.
=> I find that 1200 kcals/day is the functional minimum on any given day. Getting up to 1600 is good, much more stabilizing.
Organic, free-range everything with plenty of olive oil. I have had skillful & compassionate help with cooking since November, and it’s been absolutely life-altering — for the better, which makes a nice change!
Dr:
I’m seeing my GI doc this week. I sure hope he doesn’t retire soon.
Brain & pain
Not so good. It’ll change, but there’s no knowing just when. I’ve got a UI design & documentation project which I badly *want* to do, but I think the better part of wisdom is to write up what my training & experience leads me to envision, and find others to help do the work. Trouble is, when I get to the computer, I don’t want to write it up, I want to just do it… ADHD fail, so far!
CRPS-specific
The bone pain is having a party in my feet, legs, & pelvic girdle. Skin in my arms & legs is more burny, and it’s getting annoying. That feeling of my brain envelope being hot (not something that happens in a normal body) is a frequent occurrence.
=> Eliminating the corn (which spikes up my neuro signalling) and stabilizing my thyroid should help that a lot.
I hope.
Fibro pain
Yeah… May didn’t used to hurt like this. My joints feel like the surfaces do a quick “squish” and ooze steam at every impact.
=>Antioxidants, hydration, pacing, thyroid… and time.
Dr:
I’m seeing my primary on Monday and will ask for a referral to Brigham & Women’s pain clinic to see if we can get a better handle on this.
Ehlers-Danlos Syndrome
Ironically, the more I read about EDS, the more it explains a lot. I haven’t got enough understanding to opine further, but feel free to look it up and put your favorite links in the Comments.
Everything is in a “chase the symptoms” mode until then, and chasing the symptoms means that I don’t get things I otherwise need to manage pain and inflammation, because they trigger spasms and cause tissue tearing, both of which sound like EDS issues.
Welcome to complex chronic illness, where “competing needs” is more than a metaphor — it’s a way of life!
Dr:
I have 2 appointments, one to prep before genetic testing of a more arcane kind than I can get myself, and one to discuss results. The first of these is in November. We made that appointment last fall, so that’s really the best we can do.
Life
Best time of year is here. I hope I can get some recovery & remission, as I usually do in the summer.
The pain & brain fog keep me indoors more than I’d like, especially with the high pollen count making the histamine & inflammation situations worse. (Competing needs again: I love being outside.) It’s just too much to try to mask over all this, and I’d rather not stand out for the wrong reasons. Again.
I’ve been using my rower for exercise, when I can. That’s better for the bone pain than walking on pavement is, and I’m surrounded by pavement.
Major events
Sadly, I just lost an old sailing buddy to his illness.
Worse, I may soon lose a dear & longtime friend to hers, one of my sisterhood which formed around 2010, forged in the fires of the improbable Hell of having CRPS while being intelligent (ding!) female (ding!!) health-industry professionals (ding!!!) seeking effective care for this insane disease (DONNNNNG).
Some things you just get through and hope for the best.
Love makes everything else bearable — and that makes bereavement a stone b*tch.
On the other end of the spectrum of life… my honorary nephew announced I can expect to be a great-aunt this summer, and the first bundle of crocheted baby-gear is in the mail.
His papa, my widowed honorary BIL, is traveling the world with his skills, hard-won insight, and upright down-home charm to spread the word about what *really* constitutes good patient care. The world is becoming better for his work and I couldn’t be happier for him or prouder of his trajectory!
*Huge* yays!
=> I’ve discovered that the way to avoid emotional whiplash is to think about just one thing at a time.
Some of us are *always* living in interesting times.
Conclusion
I’m going to crawl back under my rock & lurk until all this hydration & waiting does some good. Time doesn’t do everything, but it does give other things a chance to work.
Take care of yourselves, and when you can’t do that, take care of each other. (((Hugs))) to those loved ones & spoonie-compatriots who want them.
This article is utilitarian. It provides descriptive terms for people with similar experiences to use in communicating with their doctors, payors, and loved ones.
It discusses the impact of an ordinary household task, and explains why doing such an ordinary thing could, in fact, be unthinkably difficult for people with certain neurological issues, even though their arms appear to function reasonably well.
It aims to mitigate some of the effects of the invisibleness of pain- and sensory-related disability.
Washing dishes is a problem. It’s never been fun, but it has been satisfying, because, talk about instant gratification: you do something and things are immediately better! I liked that!
Hoping for more autonomy, I recently got a great pair of washing-up gloves. Here’s what I’ve learned.
The problems with washing dishes are:
– The way water over the hands, which are rich in nerves, intensifies sensation and creates constant tactile input that multiplies every other sensation. I think it also has an effect on electrical conductivity in my hands and, as we know, the electrical conductivity in my hands is a complete mess anyway. This is where my CRPS started.
– Hot and cold temperature variation. This activates the C-fibres in my hands and forearms, the nerves that transmit hot and cold and itch and pain. My body has trouble distinguishing between those sensations. So as the water changes temperature – down to fractions of a degree, which most people would not even be aware of – my nerves and the blood vessel activity that the nerves can command are all just having a little meltdown.
– Because of histamine issues and allergies , most of my dishes are glass or metal. Both of those substances have a strong impact on my tactile sensation. (They’re hard to touch and uncomfortable to use, but I have to use them.) I think this has something to do with how extravagantly they conduct temp and, in the case of metal, electricity. Both of which translate to discomfort and pain and impair my ability to control the motion of my hands. This muscular impairment is a characteristic of long-standing CRPS.
So, between having to juggle all that sensation, all that pain, all that vascular/tactile disruption, and the loss of muscle control that comes with it, washing dishes is a real problem for me (cf. taking a shower. Another post for another day.)
Think about dropping glass and fumbling knives, and you’ll see what this means in practical terms.
My cat has learned how to respond when I break glass. She comes to the edge of the splatter zone and meeps to check in on me, then sits out of the way but in sight, supervising the entire process from picking up big pieces to sweeping the rest and finally getting up the tiny shards with large damp rags. Only then does she enter the zone and check my work! She doesn’t let me forget how important it is to clean it up properly, and comforts me considerably during the subsequent recovery time.
I got some dishwashing gloves, hoping they would help. What I’ve found is:
– They eliminate the water contact – until my hands start to sweat. Since they are necessarily an artificial substance, this happens pretty quickly because that’s how my skin responds to manufactured surfaces. The term for this is “sudomotor reflex.”
– They reduce the temperature variations, but not as much as you’d think. I’m astonished, myself, to find just how sensitive these hands are to tiny temperature changes. This relates to “thermoregulation” and “thermosensation” problems in CRPS.
– They do help somewhat with dexterity because they’re nice and grippy. However, they don’t fit well because they’re a generic size. With the quick sweating and the temperature changes, the dexterity problem really isn’t resolved.
– I don’t have to come into direct contact with the glass or metal, and that does mitigate some of these issues. It’s just that they’re not the only issues.
The peculiar nature of peripheral neuropathy with CRPS makes this pretty much unwinnable.
So I guess I still need someone else to do my dishes.
If anyone can think of a way to rinse and load a dishwasher and then remove the dishes when they’re clean and dry but still solves the problems of water, dexterity, glass and metal … I would be happy to hear it.
I’m posting this not to whine, but because it can be so very hard to articulate these profoundly abnormal sensory experiences, and I know I’m not the only one to have them. As always, please feel free to link and copy, and I’d prefer it if you point to this webpage if you put this in print or online. Thank you so much! In the end, if you need to use it, then just use it. Spoonies unite.
Speaking of spoonies uniting…
The fact that this post got written without me going into a complete fugue state and wandering into traffic, or somewhere equally unlikely, is thanks to Elle and the Auto Gnome, who kindly took dictation — and kept me from wandering off in an effort to avoid thinking about this any longer than necessary! It’s a ghastly situation and my usual coping method is to articulate a ghastly situation once, and then focus on workarounds, spending as little further attention as possible on the ghastly thing itself.
Many things are coming together and my soul is taking warmth and strength from the concatenation of care. I’m incredibly lucky — even blessed — and I feel my good fortune with all my heart. It’s a great, and unforeseen (by me), turn of events, after decades of raw struggle.
One of these blessings takes the form of a gifted young man who takes my complex & often conflicting dietary needs as a delightful challenge, rather than a terrible curse. His work with me is a hugely encouraging capstone to,
A lifetime of food-nerdery,
A career of nutrition-nerdery (not the same thing),
Decades of increasing dietary stringency,
Years of gastrointestinal fuss.
It turns out that addressing underlying nutritional needs can re-shuffle metabolic activity so that former limits are a lot less limiting.
I know, right? Who knew???
I’ve been dealing firmly with mast cell activation & histamine reactivity, by keeping everything I eat super fresh, freezing it in portions immediately, reheating in the microwave (which tastes a lot better than cooking it in the microwave in the first place), and keeping the dishes & utensils squeaky clean.
After doing this for awhile, it turns out I can eat brassicas again (cauliflower and broccoli, 2 of my favorite veg) without my thyroid flipping me the bird as it passes out.
I feel profoundly rewarded.
Competing needs: no brassicas; lots of winter veg.
Layered needs: calm down the mast cell activity & histamine responses, and my immune system is perfectly happy to take brassicas on board without trashing my thyroid in response!
Also, I was gaining weight rapidly around the time this kitchen-magician showed up; since my diet was so limited at the time (homemade parsley buns, homemade blueberry buns, farm-frozen chicken, and sprouted lentils, with only olive oil & salt for flavoring) it was very easy to do a calorie accounting.
It turned out I was in hardcore starvation mode, getting only 700-1000 kcals/day. That’s not enough. It kicked my cortisol into high gear, which is overdriven anyway due to pain & dysautonomia, and manufactured excess adipose tissue from (apparently) thin air & bad grace.
I’ve roughly doubled that calorie intake; with my kitchen-wizard’s help, I’m getting loads more veg, too, which for me are a sort of cure-all — whatever is wrong with me, it eases up if I get more veg.
Keep in mind that *any* consequence of starvation is unhealthy. Losing 80 pounds to starvation is even more horrifying than gaining them. It hurts less, but it’s more dangerous to kidneys and system function.
It’s a peculiarity of our modern sensibilities that gaining weight due to starvation is absolutely invisible, because being fat is considered so repellent (the word “gross” translates as “fat” — that’s a strong linguistic clue), that shaming & blaming is the default response, even — especially — by physicians who should know better than to disbelieve, shut down, and further humiliate their starving patients.
This obviously needs to change.
My clothes fit more naturally and my feet & legs hurt noticeably less 3 weeks on. So, that’s much better!
Competing needs: more nourishment; fewer calories & more activity, I’m told.
Layered needs: adequate calories, so my cortisol can stop screaming about starvation and let my body work better!
There will probably be a lot more about the details — why are all my veg heavily processed or overcooked? What’s the recipe for those buns? How many diagnoses am I working around, anyway? How do you get onions in when you can’t go near them raw? — but that is, as it were, food for future posts. There’s a lot more info in this topic. It’s possible there are a few books in it.
Thanks to wonderful people, I’m getting help in my home. Holy hosannahs, people, it. Is. Amazing.
My part of the bargain is to get the state to step up to the extent I can persuade it to, hoping it covers the cost.
Ever since governments realized that keeping people safely at home is much cheaper and more productive than warehousing them, sensible states work to make that possible.
Naturally, they have checklists and formulae to determine what they’ll provide, based on neat cookie-cutter notions of disability, developed in tidy rooms by people with steady pay, good benefits, and a remarkable degree of job security.
I mean… I… ay, ay, ay.
TW: Describing the usually silent reality
Fellow spoonies can guess at the blind horror it was to climb right down into the mess of this life — where getting through the day requires me to gently ignore as much as possible — and blurch it all up, but thanks to an excellent psychotherapist who knows how to pull me off the ceiling, it happened today.
Mom, it’s okay if you skip this! It’s clever & apt, but grim in parts. Keep in mind that it’s not the whole story, just the relevant hard parts, because it’s written to the task of getting money out of the system.
I separated the “Why it is like this” from the “What it is I need” and I thought this might be helpful to share with others, since I’m far from the only one who has to do this. Hope it helps.
Letter stating what my helpers do
Dear Gate Keeper,
Here is a discussion of my needs and the help provided. Thank you for taking the time to look into this.
Cooking:
Diagnoses affecting my intake are numerous and often mutually contradictory (e.g., insulin resistance & gastroparesis.) Inadequate nutrition makes everything worse, as you know. Multivitamins can only do so much.
I mentioned “no shortcuts”: this means sauces, dressings, snacks, everything, has to be made from scratch, thoroughly cooked, and frozen fresh in order to be safe. This is largely due to mast cell activation syndrome (everything super fresh & clean) compounded by the inflammatory reactivity of fibromyalgia, CRPS, dysautonomia, and multiple food allergies and sensitivities which already existed (making the cost of failure high), plus gastroparesis (so everything has to be processed and cooked.)
Everything has to be frozen in serving sizes, because the mast cell reactivity and the downstream consequences of failing to account for that are so devastating. Then those many containers have to be washed and put away. Please see housekeeping about why this is such a big deal.
Shopping: pushing a cart is like holding onto a rail wrapped in barbed wire while every bump is like a blow to the frame driving the barbed wire deeper. Not having to go through that is important for being able to do anything else in the day.
Here’s what Person A does for me:
Shopping: drives me there, handles cart, keeps us on task, remembers what I forget.
Keeps kitchen clean, functional, organized.
Keeps fridge and freezer ditto, which I couldn’t do for years (temperature, metal & glass contact; see below.)
Works closely with me to understand dietary limits and possibilities. Much learning, checking, & creative thought involved.
Preps, portions, and stores fresh food.
Makes sauces, dressings, and desserts; stores them in usable portions for me to dress my meals with.
Cooks main meals and snacks meeting my stringent needs.
Serves me a fresh, hot meal every time he’s here. Everything else I defrost in the microwave.
Portions and stores everything.
Cleans the endless parade of dishes.
Provides apt advice on how I can make my nutrition easier to access and more satisfying.
Every bite has to be cooked (gastroparesis & g.i. disorders) so this means considerably more work and more dishes.
Housekeeping:
Anything involving contact with things that affect transmission of temperature and electricity is agonizing. CRPS and its peripheral nerve activity are essentially a matter of disrupted signaling, and these are hugely exacerbated by contact with metal, glass, running water, any water at anything other than body temperature, vibration (which is brutal – imagine a full-thickness burn happening inside your tissues down through the bones) and other sensations which would ordinarily not even warrant notice, but to systems like mine are limned, imbued, and soaked in pain. Not just ouch or even agony, but a pain that causes the motor nerves themselves to fail without warning of any kind. It’s very distracting and worrisome, as well as uncomfortable and risky. It can be dangerous, as the many glass objects I’ve broken in the past year attest. Dish gloves don’t work for me due to tendon problems and what the gloves are made of.
I’m a fall risk, due to the dystonia and the repurposing of motor nerves to carry more pain. (I can supply excellent peer-reviewed articles to support all of this. If I forget to provide them and you want to see, please let me know.) And, because of the many sensitivities and reactivities I live with, packaging and serving my food in glass dishes is essential. Cleaning them is mandatory. There are no better options.
Due to the combined effects of hyperflexibility, hyperreflexia, complex regional pain syndrome and the nerve damage and “windup” that goes with it, histamine intolerance and the tissue effects of inflammation, and other factors… movements beyond very moderate range have to be deliberate and controlled, or I risk injuring myself again.
This means that things like folding sheets, reaching, or making ordinarily repetitive motions put me at risk of injury, with disproportionately bad results and disproportionately long recovery time. Amidst all this, sensory sensitivity has developed across the board. (I was an emergency nurse, mid-distance runner, hiker, rock climber, and I liked the meditative nature of housework. This current reality is hard to live with, but it is what it is.)
Here is the list of tasks Person B does for me:
Recurring serious attacks on dust and mold in the home. I havent’ been able to get treatment for these allergies to a successful degree, and they impair me badly. Dealing assertively with these environmental insults is key.
Change bed. [I’ve deleted the bit about the worst incontinence. You’re welcome!]
Vacuum floors (vibration, auditory, grip)
Vacuum baseboards, corners, overheads vs dust.
Move furniture to vacuum underneath.
Damp soapy wipe down of baseboards, shelving, & all the surfaces vs dust.
Wash curtains vs dust
Mop floors vs dust in cracks
Clean bedroom carpet and rugs in house vs mold and dust
Deep clean bathroom, bedroom, and kitchen, to keep mold levels below functional threshold.
Spot clean (I drop things often)
Fold laundry
Dishes all the time. They have to be washed really well, because of the mast cell issue.
Errands: trips to P.O., pick up meds, get cleaning products, stock up on masks, and hopefully outings when it’s warmer.
Reminders: get meds, fill med organizer, change towels, etc.
Laundry: bedding, towels, clothes, rags. I have a small apartment washer that we have to use exclusively, due to horrible reactions to commercial cleaning products.
Clean asthma gear & vital-sign gear.
Equipment maintenance for air filters: changing filters, wiping down, checking seals, etc.
It’s hard to realize, until you‘ve been through it, how very helpful it is not to be tortured by ordinary tasks of daily life. I appreciate your willingness to look into this.
Please let me know if you need any supporting documents.
I saw a whole lot of stars last night. Good for the soul, that.
I’ve been taking this opportunity to be in the experience of life without having to explain it, or articulate reasons to anyone outside my own skin. I had almost forgotten what that’s like. With very bright and articulate people in my life, it’s hard to get that in my personal life. Their need to understand is borne of pure love — they worry, because they’ve seen me through some rough times, and in order not to worry too much, they need to understand in their own minds what’s going on in this mind over here, which is in a completely different person. (Mom, you’re in good company with my lot! <3)
I’m in a lot of “thin end of the bell curve” categories, so this can take some doing: INFP (about 2-4% of the population, last I heard), serendipitously rather than linearly accomplishing (about 20%), and ADHD female (goodness knows, but the proportion seems to be growing as the markers are better understood), in addition to the weird requirements of all these illnesses — pretty much guarantee that anything normal won’t work, no matter how carefully I plan and execute.
This is the second summer in a row where things have not gone according to plan, so much so that a new term somewhere between “not according to plan” and “WTF just happened” needs to be coined to express it. I’m beginning to think I should just take this as a new life pattern, since the switchbacks tend to heal the dribbling wounds of layers & layers of PTSD. (Well-managed PTSD is not the same as resolved PTSD, although the most dramatic difference is on the inside.)
My friend and honorary BIL Ron wound up with massively metastatic liver cancer because 2 years of pandemic disruption and lousy treatment from LA’s indigent support system (which is a criminally bad system, worse than war-escaping migrant camps and most internment camps, according to the UN) left his early, localized, treatable cancer as an undiagnosed blurch on a CT scan which he had a few months before the pandemic was identified.
His care was denied because there weren’t enough staff or open beds. He was killed because of, but not from, Covid. When you think about maskless people and Covid deniers, think about treatable, localized cancer turning into a deadly and agonizing bloodbath for people like Ronnie.
Yeah… I’m not bitter… much!
Folks, this is not a drill. It’s not imaginary. It’s a fast-evolving pandemic in its early days. Read up on the Black Death for a little perspective.
A couple months ago, as people told themselves the pandemic was “settling down” right before the peak of record-setting waves of contagion and death (check the data, not the ideology) Ronnie bent down to pick something up, passed out, and woke up in hospital getting the third of eight units of blood. Then he found out over half his liver was lost to cancer and that treatment would only buy him a matter of months.
He opted to skip treatment and make the best of his remaining time.
He wanted to go fishing, so he set his mind to get strong enough for one last boat trip. His family proposed bringing him home to Northern California, where there’s glorious fishing in all sorts of waters.
Long story short, the appalling facility he was in was so good at losing contact information, that his hospice social worker didn’t realize he even had family until I had the option of including a gift card with a care package I sent from Amazon, and I included four names and numbers. Then things started happening.
If you’ve got someone in a facility, send them a card! It’s documentation that people care, and nothing happens in health care without documentation!
I never thought of it as anything other than a nice gesture, but turns out it’s a whole lot more: It’s evidence that they’re worth saving. ÷O
Put your number on it if they’re in bad shape, so the facility has someone to call. Atrocious that this should be needful, but hey, welcome to modern America! o_O
OK… maybe a *little* bitter.
Since I was about ready to have him kidnapped to get out of that stupid facility, we had contingency plans up the wazoo to get him out of there and home.
Even longer story short, it turned out that the only feasible option was to drive him home, which was a 2 person job and only one person in that elderly and health-challenged family could do that, so I changed my own plans (plan is a 4-letter word anyway) and got the soonest ticket I could.
As he listened to this planning conversation, Ronnie smiled from ear to ear with tears streaming down his face. He could take in how much he was loved and wanted, and he was going home to a slice of paradise to be surrounded and supported by the care of those who loved him.
Important note here: he already had this information, but he also had his own layers of damage which made it hard to let the information in. That resistance was there for a reason. You can say something to someone all you want, but if they aren’t equipped to accept it, it won’t go much further. There has to be a big enough change in themselves and their circumstances for those scars to shift, so the info can flow.
Ron was able to put aside everything that kept him from being able to accept that information, and he had, as the wise social worker said, “a moment of pure happiness.”
The following day, his condition deteriorated. We updated our plans to go visit and hope for the best.
The morning I was supposed to fly out, he was gone.
I did my quiet-inner-voice thing, and it said “go anyway.” So I did.
Bodhisattva oath
I’ve been contemplating the distinction between working the Bodhisattva vow and being a doormat (or codependent, as we call it now), off and on, ever since I discovered the concept when I was 12 or 13. It’s been an important part of my work of dealing with the last couple decades of harrowing illness, poverty, and systematized abuse as a patient. It’s become a regular topic recently in my meditation class. This is a big deal and an important point to consider.
The difference, it seems, is about self-care and responsible boundaries. These are particularly key for people who are women, healers, and in a vulnerable situation; it may not have escaped your notice that the wording which defines these terms was developed by men who had quite a bit of support in their work, and such people need a lot less protecting.
It’s healthful for people in habitual authority/access/power over others to embrace a practice of profound and selfless compassion. It gives them more insight and calm.
Those of us whose ground state is based on acute awareness of others require a more nuanced approach.
There are techniques which allow a diligent practitioner to pursue the Bodhisattva vow over the rim of what appears as boundaried behavior without psychological damage, but they only come after many years of serious training and discipline with qualified supervision. So, people like me have to be pretty darned careful how we proceed.
In short, I was in two minds about my own reasons for coming, but I yielded to the quiet tidal bore of my inner voice and took that flight.
Serendipity
I’ve landed in a beautifully imperfect place among people who wear their glorious sweetness and relentless flaws in flowing symmetry. From Ronnie’s kin, I’d expect nothing less.
Above all, I realize it’s not my bathtub to soak in and not a set of problems for me to fix. I’m just here as a welcomed guest and loved part of this extended & protracted family system.
This is a big deal.
There’s a lot of work for me to do (administrative nonsense, since death and life are both business matters; my trip will be paid for) and that’s healthy, because it’s easy for me and a real boon to the family. Healthy boundary there.
There is a lot of soft, verdant ground for me to walk on; a ton of stars spilling across the sky overhead; a cornucopia of Isy-friendly food pouring out of the greenery on this well-kept land; and my allergies have backed off considerably. My ex has put my health needs absolutely first in every consideration and the rest of the family is happy to support that. Definitely healthy.
And me? I’m not over-explaining! It’s amazing :D! I just quietly take care of my needs and appreciate everything that I *can* partake of. Good boundaries there, too.
I’m learning, carefully, again, how to be present. How to unlock from anxiety without letting go of my real needs. My phone is nearby and in signal, but usually off. That’s healthy too, right now. It’s a kind of technology break, which my battered and hyperactive brain is probably long overdue for.
I’m also bereaved in the presence of others who are also old hands at bereavement. It’s a peaceful thing. It feels curiously wholesome, even as grief and mortality are shredding sorts of events. Ronnie and all our late loved ones are very present in their very absence.
I could natter on about the wheel of life and possibly even spout some Buddhist wisdom about interconnectedness and emptiness, but to put it in words is to miss the point. It’s an experience. All you can really do with an experience is to be in it and allow it to be part of you.
So that’s what I’m doing. And there’s real healing in it.
For some things, no explanation is needed because, at root, none is… oh I don’t know… possible?
Anyway, I’m OK. I’m doing the things and being the me and accepting the limits (including transport) while appreciating the strengths (like interconnectedness) and feeling very secure and centered and remarkably peaceful withal. This is good. And if my phone is off, be assured it would be on if I needed it. Right now, the stars and the green and the peace are healing me, and I’m simply letting them. <3
Ladies and gentlebeings, here’s what I’ve come to after a 6 month period of, firstly, a strict diet of tapioca, carrots, butternut, apples, and chicken; then, careful reading about *tested* foods on *living* humans, plus extensive empirical testing on my own particular system. The fruits (, veg, herbs, and meats) of this work lies below. Foods that I currently remember as improving the histamine picture have a +.
Note: I’m focusing on what I *can* eat as part of a low-histamine diet. Where my diet is restricted for other reasons, I say so, in order to point out where there’s obviously something for others to explore.
I don’t mention higher-histamine foods nor do I go into the details of what makes a food low-histamine (which can involve mast cell triggering, histamine levels within the food, salicylates, non-food triggers that raise the background level of reactivity, whether fermentation or aging is inevitably part of the process – as with beef – and so on) because that’s a whole ‘n’other article, and a bit beyond my bludgeoned brain at the mo’.
Caveat emptor: we’re all a bit different. This is why empirical testing, tracking results for yourself, and being able to notice when things change, is so important. My list is basically ok in principle, but it won’t be right for everybody, and may not even be right for me in a couple of years.
Besides “everything organic” and “everything fresh”, the third leg of this mow-histamine diet is “everything freezable frozen”, because leftovers and meats start making histamines real quick. So, freezing and then defrosring in the microwave is the only safe way to go with yhese things.
I let stuff that’s fresh off the stove or out of the oven freeze up on the top shelf (usually atop the “buns” box) and then move it to its rightful place:
The magic lists
Everything, absolutely everything, is super fresh and organic. This is part of the deal with low-histamine foods, and I’m ever so grateful that it’s possible right now. (Thank you to the federal SNAP/Food Stamps system and to HIP, the produce-enhancing state funding system for low-income people, plus an outstanding local farmer’s market that works with these programs!)
Produce:
+Apples, fresh local low-spray or organic (by low-spray, I mean they get sprayed twice, once when the buds set and once when the fruit sets. I find I tolerate this just fine, as long as the apples aren’t sprayed for storage)
Fresh cider, UV treated to impede fermentation (when I’m not frail)
Blueberries, wild
Cranberries
Peaches, when not frail
Plums, most kinds, when not frail
Cherries, when not frail
Mangos (not bruised)
Spring onions (some people are good with sweet white onions but not spring onions, and some can’t tolerate any onions, so YMMV)
Garlic heads (as above)
Sweet peppers (I find red bells and bullhorn peppers easiest to digest)
+Asparagus
Cauliflower, if good (no black or yellowed spots)
Soft/summer squash: marrows, zucchini, yellow crookneck (scoop out seeds if currently fragile)
Different squash: delicata, pattypan (seeded as above)
Beet greens
Radishes (which I like to steam)
Celery
I can’t eat leafy cabbages because my fragile thyroid poops out if I do: mustard greens, collards, chard, bok choy, napa, savoy, radicchio, kale, green and purple cabbages, and other winter-harvest yumminess! Check them out for yourself, as long as your thyroid and gut is up to the job.
Protein:
Chicken, turkey, pork, lamb (frozen straight off the block; another farmer’s market item here) (NOT ground: that generates histamine, possibly from the extensive cell damage)
Eggs (from scratching, soy-free hens)
I can’t eat lentils, beans, or peas due to gastroparesis, but you lucky so-and-sos who can might want to read up & experiment to see which ones are ok for you.
Lipids:
These have to be fresh and not have any whiff of rancidity. Since all my food is fresh now, these and my protein sources are my only source of lipids for my brain and spine:
Olive oil
Grassfed (or Kerrygold) fresh butter, not raw
Avocado oil
Drippings from cooking meats, frozen right out of the pan. These are *wonderful* for cooking veggies with!
Coconut oil (when not frail)
Carbohydrate rich:
Rice (plain whites, basmati, or jasmine are all ok for me; brown and sweet rice are not for frail times, but ok in small doses at other times)
Sweet potatoes, any kind but Japanese (which I think I did to myself by eating them too often at one time! Darn it)
Tapioca/yucca/manioc, same vegetable; fantastic for a sluggish gut & delicious made with apple cider
Farmer’s market honey
Sugars: panela, jaggury, coconut (all of them unrefined & mineral-rich, so YMMV)
Beets – with greens (I use the stems to flavor soups and I steam the greens or drop them on top of a batch of stir fry; delicious!)
Carrots, lots, as they go with everything
Broccoli
Parsnips, if I’m not currently frail (they’ve got such good nutrition I keep them on my shopping list, but they’re the first to go if I’m not up to the mast impact)
Celeriac
Hard/winter squash: butternut, acorn, kabocha (NOT pumpkin or spaghetti squash)
Rice is my only grain. Some do ok with sorghum or buckwheat or some other things, but it’s hard on me in anything but small doses & when I’m not reactive.
Flavorings and spices
I can do, almost all fresh:
Parsley
Basil
Dandelion greens
Cilantro
Sumac (this is dried)
Bay leaf (dried)
Rosemary
Sea salt
Mined salts: Kosher, pink salts
Garlic
Ginger
Turmeric
Cedar sprig (fantastic when cooking chicken or buttered black beans, not that I can eat the beans any more)
Cumin (when not fragile)
Here’s the fun part…
Recipes
The web is international, and I try to work with that 🙂 Please be aware that, as my cooking was learned in US-origin households and restaurants, I cook by volume rather than weight. Measurements are noted accordingly. (I’m aware of the flaws in this system, so I use recipes that can accommodate the “fudge factor.”)
These are much-loved ingredients I make ahead:
“Ginger Fabulous”
I almost took a picture of this, but it just looked brown on camera. It’s lovely earthy honey-colors IRL.
Peels from 4-6 apples (may freeze ahead)
Ginger x6-8 thumbs (a bit bigger than my smallish thumb, anyway)
Farmer’s market local honey, ~1/2 cup [120 ml]
Sugar (panela or jaggury for me; light brown or raw is probably good), same volume as honey
1 pint [500 ml] cider
Optional: Dash of clove, if you’re ok with it
Slice ginger to 1/8″ or less.
Chop apple peels to about 3/4″ segments.
Put everything in a good pot.
Simmer until all the ginger is translucent, usually ~ 1/2 hour.
Let cool.
Try to keep enough for later; I find it hard to stop taste-testing. Uses:
Use as is for preserves, or process/blenderise to rough texture for marinade, jam, or even hot drink if you don’t mind a bit of dessert in the bottom.
Chop parsley and the leafier part of dandelion greens to 1/2″ lengths.
Pick basil leaves off stems and chop a bit smaller than that.
(Wrap the stems in foil and keep in freezer for flavoring soups, as their flavors cook down delightfully.)
Throw it all in a processor and chop very fine. (I have to go 1 head of parsley & equivalent of others at a time, because my processor is not that big.)
Package up into ice trays, or in foil or paper by ~dessert spoon or ~50 ml sizes and freeze. Uses:
1 of these dresses 2 to 4 scrambled eggs or omelettes, depending on taste.
I take a batch and mix it with softened Kerrygold/grassfed (not cultured!) butter, to a ratio of 1 butter : 1 pressed-down greens by volume, and beat well into a super healthy spread. I refrigerate enough for a few days and freeze the rest. Way more yummy than something this healthy should be!
“Isy’s elf-rising flour”
This recipe is taken from alittleinsanity.com, but I removed the xanthan gum, use non-fungal risers, and make with organic flour ingredients. Its ingredients are friendly to systems dealing with inflammation and histamine problems. It makes buns, quickbreads, and muffins very quick & easy to put together. (I haven’t tried it with pancakes because I can’t limit my intake of pancakes sufficiently & don’t like to feel that sick, so doing without is my best bet rn.)
This recipe uses weights because, for the most part, the ingredients are often packaged in these sizes so you just dump out a bag of each. Easy!
24 oz [0.7 kg] brown rice flour, fine
24 oz [0.7 kg] white rice flour, fine
24 oz [0.7 kg] sweet white rice flour
20 oz [0.6 kg] tapioca flour/starch (same thing)
2+1/2 [37.5 ml] Tablespoons baking soda
1 Tablespoon [15 ml] baking powder (I push this through a tea strainer to get all the clumps worked out. I abhor the taste of baking powder clumps)
2 Tablespoons [30 ml] salt
Blend carefully in a huge pot. I use both a paddle and a whisk, gently.
Take the time to get everything *very thoroughly blended*.
This makes a gallon plus 1.5 cups, or about 4 liters.
Uses:
This makes a forgiving dough, and will generally work out fine.
2.5 cups [or about 750 ml] of flour will take:
5 to 7 tablespoons[75-100 ml] of butter (maybe more; tell us if you try it?)
1/3 cup [80 ml] liquid
1/4 cup [60 ml] to 1/2 cup [120 ml] of sugar
Eggs, 1 to 4…
If you use 1 egg per 2.5 cups of flour mix, it gives a texture suitable for scones or gf (American) biscuits.
If you use 3-4 eggs per 2.5 cups of flour mix, it results in a soft, puffier texture with more volume, as for quickbreads [teacakes] or (American) muffins. Additions
It adapts well: you can use water, broth, milk, or cider as the liquid, and can add as little as 1/2 cup [120 ml] or as much as 1+1/4 cups [300 ml] of diced chicken or Super Greens or wild blueberries – with or without some Ginger Fabulous – and still get a wonderful result.
It bakes in 12-15 muffin tins (depending on the extras) at 350*F [175*C] for 16 to 20 minutes in my oven, or until there’s no steam in the scent from the oven / toothpick comes out dry.
Here are chicken buns & blueberry teacakes in their freezer box. Defrost & warm by microwave on low for 30 seconds on top and 30 seconds on bottom.
I’m still working out a recipe for lembas, but it’s only a matter of time. Buns made from this are light & crumbly all right, and certainly very filling!