Once upon a time, I asked my hot-shot pain specialist (I’ve had some real rock-stars) for something heavy-duty and intense (I forget what).
He told me that he wanted to stick with using current meds a little differently and upgrading my self-management skills, because I had a lot of years left and he wanted to keep something in reserve for when things got worse.
This doctor really understood long-term palliative care — palliative care meaning, you’re not expected to recover, so treatment means managing symptoms for as long as possible.
That’s not about dying comfortably, most of the time. It’s about living anyway. Being sick is not the end of life. It’s just a heck of a detour.
He was apologetic and sympathetic, hoping I wasn’t too dismayed and disappointed. I was delighted to realize this physician firmly intended for me to have a long and active life, and was asking me to step up to the plate to help to make it so. I don’t think he realized that, in that moment.
I said to my specialist, “My job is to figure out how to get through my days as gracefully as possible. Your job is to hold the long view for me, and figure out how to manage my care over time so I can get through the years as gracefully as possible.”
He looked at me in perfect stillness for a long moment. For someone who likes talking as much as he does (for good reason; interesting talker), that was weighty.
He asked, “Would you please come to my severe-pain support group and say that?”
Sadly, I really couldn’t drive safely that late and knew I couldn’t get a ride for it. (This was pre-pandemic, so, no remote possibilities.)
It’s possible that he was as frustrated and disappointed that I couldn’t come and say this to his patients as he had expected me to be about the medication. So, Dr. Saberski, this one’s for you!
Emergency visits
The purpose of the Emergency Department (or A&E/Casualty, for the other English-speaking countries) is to figure out if anything is going to kill or disable you in the next 24-48 hours. It’s a very specific remit.
Flare-ups of chronic conditions can creep into that remit, severe pain being very disabling in itself.
However, another condition of mine, gastroparesis, is not a great candidate. The heavy-duty pain meds in the ER are mostly narcotics, which rarely work for intestinal pain and, more importantly, make the intestinal paralysis worse. The anti-vomiting meds may not be better than what your doctor prescribes, although they may be different and worth trying for that reason alone.
ER nurses used to have an effective line in moving stubborn bowels. It seems this is no longer the case. It’s often considered a specialist task, not that specialists do it either. If in doubt, look up “soap-suds enema” and follow the instructions carefully. Stay near a toilet for the next 6 hours as your guts remember their job.
It’s vital to know that dehydration can be deadly or disabling, and the ER is exactly the place to go for treating that. So, if you can’t keep even sips of water down for a day or two, for any reason, and you’ve got the sunken eyes and play-dough skin (pull up a little fold on the back of your hand, and it stays there), the ER is the place to go.
Bodies can’t recover without water. Water really is life.
If your condition requires specialist knowledge to treat, but probably won’t kill you or further disable you in the next 24-48 hours, the ER can be bitterly frustrating, because thats not their brief and it feels unfair to ask them for it when they don’t have the training or funding.
However, it’s perfectly okay to phone them up and ask the triage nurse what to do. I’m an old triage nurse and I loved it when people were “on it” enough to call and ask. If they didn’t need to come in, I could tell them what to do and what to report if things changed. If they needed to come in, I knew they would do as well as possible and I could get them sorted and into appropriate care faster and with a rare smile on my face.
Being deliberately involved in your care is that powerful a message to send to your system. We can’t consciously control our systems, except in nudging things here & there, after specific training. We can deliver primal shoves with our basic approach, with how deliberate and mindful we are about our care.
Urgent care
Urgent Care is where you go if you’re pretty sure you aren’t going to die or be (further) disabled, but you do need same-day care.
Keep in mind that these providers do not have specialist training, but might be able to make a call to your specialist or be willing to discuss what you want from them. I said “might” — it depends on factors beyond your, or even their, control.
In the US, they usually can’t make referrals — except to the ER, if they find that you need further scans or a higher level of care.
It’s not fair to them to expect specialist care. That said, it’s not fair to you to have an inaccessible specialist. Lousy situation.
Primary (general) care
This person is supposed to be the ring-master who holds the ends of all the threads of your care. They’re supposed to take over your prescriptions (unless they’re actively in the “figuring out what works” stage) or you’ve got a specialist who wants to stay absolutely on top of things.
This is the person you usually call for coughs and colds, annual checkups, questions about whether you might need another specialist or different care, and when you want to talk over health care concerns, including confusion with how the system works.
They’ve still only got 5-10 minutes with you, but it’s time well spent if you’re confused or overwhelmed. As ever, note your issues and questions before going in, to make the best use of your time together.
One of the uses of those “talking” visits is for a medication review, one of the best uses of time there can be for us. See the Pharmacist section for more.
Pharmacist
These are the medication bosses. Their depth of knowledge of medications, interactions, side-effects, and alternatives is absolutely daunting. They’re the wizards of meds.
If you’re having symptoms that might be side-effects, this is who you ask about it. If you’re unsure about a new med or dont know what to expect, this is who you ask about it. If you’ve got genetic variants that might affect medication metabolism, this is who you ask about it.
Medication review
If you’re concerned at how many meds you take, talk to your pharmacist first. Then, with the notes from that conversation in hand, talk to your doctors.
This is called a “medication review” and everyone can do it annually, or more often if things are changing for you.
Pharmacists can’t prescribe, because the depth of knowledge about various bodies in sickness and health is the reason why physicians spend even longer in training than anyone else. Most of medical care is beyond medication. It’s why nutrition and self-care matter so much.
The body is its own unique thing and needs its inhabitant to be involved for best results.
In short
Medicine is really, seriously deep and complex. Each of these segments of the health care system is necessary, and none can substitute for the others.
It’s an imperfect system. It should be much better, but, heaven forfend, that might cut into enormous corporate profit margins. Patients, doctors, pharmacists, and every actual helping human has to work within the restraints of enormous corporate profit margins.
I’m going to give organizing my mental database a try here. The aim is to pick one broad topic each month and cycle through them in a year. I’m doing it the way nurses and doctors are taught to do it: head to toe.
Physical assessments have to go from head to toe, every time, without exception. This makes use of the brain’s basic tendency to work in patterns. If you assess every patient from head to toe, every time, then the variances are easier to find (because your brain is so dialed into what to expect at that point in the pattern) and it’s a lot easier to get to a sound differential diagnosis.
If I go to the doctor with a sore knee, the doctor is still going to notice my level of consciousness, attachment to or detachment from my environment, track my gaze and whether the sides of my face are more or less equal, differentiate how much of my limp is because my knee hurts and whether any of it is because my balance is off (all of that is about the brain), notice my breathing pattern (lungs), become aware of blood- flow problems (heart) showing up in my skin, and checking to see if I’m “splinting” or bracing against pain or weakness in my abdomen (g.i/g.u. systems) and hips (ortho, right above the knee).
An experienced doctor does most of this in 1 to 3 seconds, because it’s a head- to- toe assessment every single time and they can just let their pattern-matching brain (which is powerful and primal) take care of it and send up a flag to their conscious mind if anything is abnormal.
The medical term for “head to toe” is “cephalocaudal”, which literally means “head to tail”… but humans don’t have much in the way of tails, and our bodies keep going for quite a ways after them. I’d love to hear from my Latin-knowledgeable readers what the term should be!
I’m recovering from a migraine, which is very on-topic, but I’m not yet up to writing much. I thought I’d introduce this new structure, which I hope will be a bit simpler and less overwhelming than “what am I wrestling with right now that I could usefully write about?” There’s so much to write about, it magnifies the intransigence of the empty page. (Writers know what that’s like.)
I was chatting with a close friend about a week ago. He’s placed to be on top of current events with a depth and nuance that my vomit reflex can’t stand. We had an interesting conversation which was mostly me chirping, “But what about…?” And him giving me a really good update on stuff I’d never be able to stay upright long enough to research.
My brain was twinkling away on the incoming tide, sorting the info and soaking it into the correct metaphorical tide-pools and littorals.
I soon realized that, though I was sorting words coming in, I was having a terrible time getting words out. I didn’t realize, until that moment, just how completely that parsing a thought may feel verbal, but might not be.
I thought I was wording just fine as I thought, “okay… this goes here with news ownership; this goes there with political gamesmanship from Brand X; this relates both to Brand Y and legal process” and so on.
On the outward flow, all I could get going was along the lines of, “so, uh, how’s the… thingy… you know, from… what’s-his-name…” and I realized I sounded immeasurably more mentally inept than I felt.
I wanted to say, “look, I’m still in here and I’m taking in everything you say. I just can’t operate the outgoing current right now and my word capturing is going great, but my word finding seems to be underwater.” I could not fund the words, of course.
It’s been grimly fascinating to me to find the many ways a brain can go off-line in bits & pieces, and how my mental activity and neurological activity have these unthinkably complex ways of associating and dis-associating within themselves and between each other.
Everyone’s brain is linked up in completely unique ways. Just imagine what it would be like to work with people who could relate exactly what is and isn’t working and when. It’d set off such an explosion in the advancement of knowledge that.. wow.
A pointless note of wistful longing
It’s a real pity I can’t handle any schooling, let alone medical school, because this is exactly what neurologists need to know about to make their lives – and, boy howdy, ours! – a lot more useful and interesting.
As it is, patients are considered inherently unreliable in the medical mind, and, although that’s extremely insulting, it’s not crazy within physician context: the precision of thought and accuracy of terminology is rarely there, because so much training goes into commanding the information the way a doctor does.
Conversely, it’s adapting through a traumatizing cascade of brutal experiences that creates a skilful and well- informed patient. Training that’s so high-level it amounts to nosebleed seats for one; autodidacticism that makes Richard Francis Burton look like a playboy (oh, wait..) for the other. (When I can find someone who’s as brilliant an autodidact but not a moral negative, I’ll revise that sentence.)
It really is a different language and these two rather fragile mind-sets have trouble reaching across the cultural gap. (Anyone who thinks doctors aren’t fragile should just try correcting a few. It can get rough.)
I think the ratio of truly secure doctors to the rest is about the same as truly adept patients: they are definitely around, but can be hard to identify even when you’ve got one. It takes hard work and a lot of fearless honesty in both cases.
Buckling on my helmet. I’ll get it from both sides now.
The onus winds up being on the traumatized patient, who usually has more clock-time to prepare for the visit. The doctor has to turn around and deal with someone equally intense in 2-7 minutes, so they have to stay mentally free to do so.
Yes, let’s hear it again for corporate medicine and its unholy offspring. So efficient, such a great use of limited resources… not.
There isn’t (yet) a cultural context in the field for cross-training as a patient and as any sort of licensed practitioner. That’s the key deficit.
Practioners get culturally demoted when they become patients (which is disgusting, but predictable in such a heirarchy) and patients get shoved into a little cultural pocket for things that fall between weird and interesting without fully qualifying as either.
Fun, eh? It’s one stellar example of the waste in the system.
I’m working on building up stamina because being a blob doesn’t agree with me.
I had one of our rare, hard-won, absolutely stunning neuro physiotherapy sessions yesterday. It usually takes time (days or even weeks) for my body to embrace the resetting, but this one is showing up fast.
Until last week, walking a bit too far would wipe me out.
When I was well, walking lifted my spirits and calmed my mind, and “too far” had more to do with comfort & convenience than anything more pressing.
For most of my illness, walking helped in the aggregate – if I kept it up, I did better over time. It was good, and I was glad to do it, but…
I’d forgotten, until today, just how lovely it was possible to feel after a good walk.
Yes, I’ve overdone a bit, and I’m open to the idea of staying in tomorrow & taking it easy.
I just… I haven’t had a workout high in… dear heavens, I can’t even remember. Decades, possibly.
Must remember to send this link to my physiotherapist. She’ll be:
A. Over the moon for me.
B. Reminding me to drink a lot of water and put my feet up for a bit.
It’s hard to keep it all in perspective – to celebrate this properly, without falling into the old trap of ignoring all the ongoing work it took to get here; to keep it up & stay honest about the jungle of limits I still have to negotiate.
Good day, though, eh? Really, really good. My heart is as light as the feather of Ma’at…
Without descending into the morass of modern U. S. history and politics, let’s just say that I’d like the first months – up to half a year – of the new regime to happen with me being somewhere bearable, where good produce is a lot cheaper and the medical care both stable and affordable.
None of this is likely here, where my food prices rose about 30% during the harvest season and there is much loose talk and planned chaos around Medicare and the dole (which I depend on to stay alive) – not to mention the cost of everything rising by 15-60%.
The pundits and those who follow them tell me not to worry, because there are rules and procedures “they” have to follow.
Given the Mump track records regarding rules and procedures, all I can do is smile sweetly so as not to worry my loved ones, and let my mental gears turn more quietly.
Hot tip #1: a tariff is a tax. These get passed on to the consumers, not sucked up by the companies from countries exporting to us.
Hot tip #2: as we’ve seen so clearly over the past 5 years, industries don’t just raise costs in line with their own expenses, but jack them up to see just how much the market will bear. Given a captive market, this has gotten really ugly. Remember eggs last year? The sub-prime lending fiasco leading to the 2008-9 crash? Yeah, it’s an established pattern.
So anyway… here I am: if I stay in one place, I’ll be wrestling hard with un-meetable expenses (my dietary needs are simple, but not cheap) and a constantly-cycling urge to run away. That’s neither stable, healthy, nor fun. Been there, did that, threw away the t-shirt.
I didn’t grow up in one place, or even one country. I’m not mentally stuck here, and I don’t believe I have to put up with the scrambling anxiety or insufferable expenses to come as the Mump Regime and its trail of chaos gets itself through the initial reality-checks.
I’ve been toying with the idea that it’s healthful and good to be warm, stable, and happy. That takes adjusting to, because so much of what makes me feel anchored to the world is about work. I love to be productive. It makes me feel superbly grounded to be useful/helpful to others. This is very compelling… but as far as my daily choices go, doesn’t have a lot to do with being warm, stable, and happy.
It does have to do with abusing my eyes and attention with falling down back-lit rabbit-holes and trying to turn the swarms of information floating around in my brain into streams of relevant words, pertinent to the question I’ve just read.
But I’ve got serious limits and, as it turns out, I am much more useful and productive after I’ve been taking really good care of myself and playing and recreating and being happy outdoors – a lot.
This doesn’t sound like computer-gazing, which is how most of my work happens.
This focus on making myself happy is a weird concept, and I’m still working out a lot of the details. I mean, not even details – I haven’t settled on where to start; even my departure date is unfixed. Getting the right people in to keep my place clean & warm while I’m gone is kind of a big deal too. I’m not prepared to move and won’t sacrifice my sweet little home – not until I’ve got a much better offer in hand, anyway!
Anything could happen. I’m trying to keep breathing properly as I say that.
I’m profoundly curious. (Take that however you want, LOL)
When I was an inch from dying, around 12-14 years ago, when there was nothing left of anything I thought made up my life… I found, down there at the bottom of everything that had been, this relentless creature who had to know how the story would go. I could not allow death to overtake me because I’d never know. So I lived – on pure willpower for a while, but then things started to change and get better & better.
This came up in my Pain Psychology appointment today, following on from the “new pain doc” appointment I’d had the day before. I’ve had 4 pain specialists in 9 years, and (thanks to extended litigation) around 19 in the past 20. Since much more than my life depends on my pain docs, and I have no control over the situation, this is harrowing, every single time.
My medical PTSD is a main focus of my pain psychology treatment, which is how this came up for discussion.
My curiosity is clearly more fundamental than my reflexes and primal needs, so, “Let’s figure out how to use it to interrupt some primally-driven anxieties.” Today’s quote from Kylie Steinhilber, PhD, my pain psychologist. From this, we discussed 2 further insights:
Being inquisitive is about holding an empty mind/heart in the present: pure now, with an open eye to the unknown future.
Trauma responses are about having emotional context and re-experiencing that history, thinking (“knowing”) it will go this way or that way based on what’s happened before.
I’ve never realized that quite so clearly.
If this had been a rough “new pain doc” visit, I could go to the open & curious state of, “so that’s what’s here/now. I wonder where it will go?” – instead of falling into the misery and grim anxiety of “knowing” what it will be like based on prior experience.
Note to self:
BE CURIOUS about where the story will go! That is rational, even though it doesn’t come with a plan.
Prior experience matters, but it’s a lot better for me to stay open and inquisitive and be with what’s going on now. More options, less antipathy between us, and that opens up communication – which improves outcomes, even in a crap situation.
Serendipity was my brain’s home base pre-injury, & it likely still is. It’s OK to go there and hang on when things get uncertain.
I’m in the 20% of humans who thrive through a serendipitous approach, although it drives more linear people (the 80%) up a tree, because it looks crazy to them & sometimes makes them want to reach for a net – or a straight-jacket.
When I use their (the 80%’s) linear approach (which I’m technically good at; mad skillz), the best I can do is mediocrity, if that. It doesn’t work well, no matter how careful the planning and research I put into it. Makes no sense, but that’s how it goes.
Chaos and WTFery are going to find me. I’m one of those people that things happen to. No, that’s not logical, but accepting it is rational. Interesting distinction between logic and reason there.
I see my mental job as learning – over & over – how to ride the metaphorical wild horses, not keep trying to dodge their flinty hooves as they run over my well-plotted garden.
20% of humans are like this. We’re not alone, just unusual.
Note to self:
I CAN TRUST MYSELF to know how to go and when to stop. Truly.
Cf. my “15% overdo recovery time” note in my personal pain rating scale. I really do know what it means to overdo by 15%, and why it’s harder to recover from than 10%. *That’s* evidence of a high level of insight & self-management. I can perceive it accurately when I loosen my grip on “tha Plan” and listen to myself.
I said to myself, “Self…
“LET the inner story that ‘everything will go wrong’ BE WRONG.”
Some moments suck anyway, but they pass a whole lot faster when I stay curious and open and let things go differently than expected.
All that said… I am simply over the moon with delight that this “new pain doc” visit was such a good one and that I feel safe at last in that part of the system! That frees up a ton of energy, now and ongoing. The relief is stupendous.
The resident (training) physician remarked, unprompted and naturally, “After all, you are the expert in your own body.”
Hearing that from a doctor is a show-stopper. As one friend & compatriot said, “I’d be less surprised if a unicorn came to your door and told you you’d won the lottery.”
I wrote the start of this for a fellow spoonie today and realized it’s a good starting point for a subject most people find overwhelming: reading medical science when you’re starting off as a non-scientist.
The article I cite first is a good example to start with, because it’s written well and has passages of clear English to work with. So…
I suggest reading the abstract and introduction. After that, just skim the first sentence of each paragraph, since (in science writing) that tells you what the paragraph is about.
If the first sentence makes no sense, skip that paragraph.
If you can figure out the first sentence, glance at the rest of the paragraph to see if there’s any more to glean. If not, move on..
It’s a skill
Reading science is a skill, and skills take time to master. That’s expected! Share what you glean with your doctor and ask them to help you understand it better.
Honestly — this isn’t to puff myself up, it’s just the nature of patients to dis themselves, so hear me out — if you can read my stuff and make out half of it, you are plenty smart and literate enough to start reading science. It’s just work and time, and the time will pass whatever we do, and the work will get easier with time. We just have to take care of ourselves and pick our time, when we’re chronically ill.
Using the right amount of honey
Doctors might give you attitude about comparing your Google search to their medical degree, but that’s not what you’re doing: you’re studying up on your condition, which is wise, and you’re expanding your info base on this thing that has imposed on your life, which is survival.
So, feel free to correct them sweetly, and don’t be afraid to pour some admiration on them if it helps them to re-focus on your information-gap.
The point is not who knows more overall. That’s not in question. When you talk to your doctor, you’re talking to someone who had to memorize, for instance, the Krebs cycle (here’s a partial explanation: https://www.medschoolcoach.com/the-krebs-cycle-mcat-biochemistry/) — so, yes, they have a depth and nuance of knowledge that’s nearly impossible to replicate without going to medical school.
They like having that acknowledged, because they take a lot of painful flak for not knowing everything about everybody’s illnesses all the time, and they need to know that you know what an effort they made to be able to work as a doctor.
So, it’s good to acknowledge that enormous effort.
Then they are usually able to hear you when you clarify that you’re not arguing with them, you’re trying to improve your understanding of this thing that affects you so profoundly. You trust them to help because of their knowledge.
Trust. Help. Knowledge.
These are keywords because they are core professional values for most doctors.
They’re important to acknowledge, and great to invoke and rely on.
That said… if you can’t rely on these characteristics in your doctor, even after you tell them that that’s what you need, then it might be time to find another doctor if you can. These core values are far more important than whether a doctor has good social skills or a good handshake.
When all is said and done, guess who has to live (or not) with the outcomes? It’s you. While the doctor is the subject-matter expert on the medical info around your condition, you are the subject-matter expert on being in your body and dealing with the fallout. There’s a degree of respect that should go both ways, though modern practice makes that hard.
The key to reading science is realizing — or at least, going ahead as if — you’re perfectly capable, and just need to practice. Science is written by humans, and you’re a human too.
1. You are a perfectly sensible person. If you’re reading this, you know how to read (or access translations from) English; also, you have access to a whole world of dictionaries. MedlinePlus is especially helpful in explaining concepts and helping us learn to read medical stuff.
2. Not all scientists can write well in English, and none of them write in English all the time. That’s okay. They went to school for a long time to get extra vocabulary and learn to do what they do; good for them. They’re still people, and they have to write in English at least some of the time. That’s where you can come in.
3. You can read the English just fine. Trust yourself and take time. With practice, you can learn more lingo over time, and get better at reading more science.
Just work from what you can understand now, and let that grow over time. You’ve got this.
Choosing credible sources
While you’re learning to read science, start where you can and work from there. As you get more confident and your understanding grows, you’ll learn to be choosier.
The gold standard for science info
When learning how to assess science, you’ll hear a lot about placebo-controlled, double-blind studies and that method is often important. This method of science gives us more reliable statistical probabilities about whether something will work in a certain situation. The statistical probabilities become reliable when several thousand people (“subjects”) have been tested, probably over many different studies.
With rare diseases, this is obviously pretty unlikely, so we have to work with less scientific certainty. C’est la vie.
Statistical probabilities have more limited value for patients than doctors, because we’re individuals, not pooled data. There used to be a phrase used in medical school: “Statistics mean nothing in the case of the individual.” This has gone by the wayside a bit, but it’s still true.
We may have to cast our nets further afield, because we’re looking for clues that might help us, personally. Be aware when you’re doing that, and put those science reports in your mental “hmm, maybe” folder.
I showed a case study that had a marvelous impact to one of my best doctors. He said to me, “If I could put that effect in a bottle, I would. It worked for that person, and we have no idea why. We do know that it doesn’t work for all these other people. Everybody’s different. Figuring out how to apply one thing to help a lot of people is our holy grail!” Lloyd Saberski, MD.
And that’s why doctors rely on the pooled data gathered from the scientific method. They want to help as many people as possible with each thing they try. Otherwise they fear they’ll spend too much time chasing rainbows.
We patients have to find our own rainbows, just as we have to count on our doctors to keep an eye on what’s statistically worth trying. It really is teamwork, and we both need to do our jobs.
What’s peer review?
Before you give a study to your doctor, it’s worth checking if it’s from a peer-reviewed journal. Don’t expect them to put too much stock in it otherwise.
Peer review means that other people in related fields have checked it over for sanity and validity. This is important for us patients, as well as the doctors who rely on the information.
You can Google whether the journal your article was first published in is a peer-reviewed journal. JAMA, BMJ, and the Lancet are all reliably peer-reviewed.
The value of literature reviews
Then, after a fair amount of studies have been done on a topic, there’s usually a literature review. This is when a qualified scientist takes a close look at all the studies, throws out the ones that were badly designed or poorly run (because bad technique creates bad data. “Garbage in, garbage out”) and writes an overview of what the current good science says.
They also discuss the strengths and weaknesses in the data, and suggest where future science funding could go, in light of the science so far.
Literature reviews are wonderful places to improve your knowledge of your disease/condition, expand your vocabulary, and get a lot better at understanding what goes into the science on your condition in the first place.
For instance, it used to be widely believed that most people with Complex Regional Pain Syndrome had had traumatic childhoods. (“Blame the parents” LOL.) There was a literature review done on about 30 years’ worth of studies, and it turned out that almost all of them were so badly-designed, poorly run, and calculated with so much bias, that nearly all of the studies had to be thrown out!
This taught me very important lessons:
– Just because most people say it, doesn’t mean it’s right, even if they should know better. This is an excellent attitude to have while reading science.
– Methods matter. You’ll learn over time how to sense whether the methods used are appropriate to the topic studied. The wrong method can lead to truly bogus results. The method has to fit the material.
– People lose their minds when they think about pain, as well as when they think about childhood trauma. In practical terms, this means I have to approach all normal (non-CRPS) people’s reasoning about my condition (which is characterized by relentless agony which a non-CRPS’d brain cannot even conceive of) with compassionate criticism. They do not know what it’s like, nor how to live with that pain and still think rationally. They’re not able to know. I don’t want them in a position where they do know, because that’ll mean their lives are as battered as mine is.
Therefore, every word they say has to be filtered through my awareness of how their minds get lit up by unreason, when they think about my pain. This, believe it or not, is perfectly natural. (Look up “amygdala hijack” for background on this mechanism.)
I survive because I’ve learned to substantially displace or ignore one of the most powerful primitive signals in the human body. That isn’t natural, and nor should it be.
These scientists mean well, without question. However, their logic is necessarily fractured when thinking about this, because they lack my tools for facing it. I need to dig into their data and methods before I can buy into their conclusions.
That’s good to know!
The conclusion of that literature review? CRPSers are likely (not guaranteed) to have had relatively eventful lives. Whether the events were traumatic or wonderful wasn’t relevant to our probability of developing CRPS.
In other words, we live in interesting times!
Where to find science to read
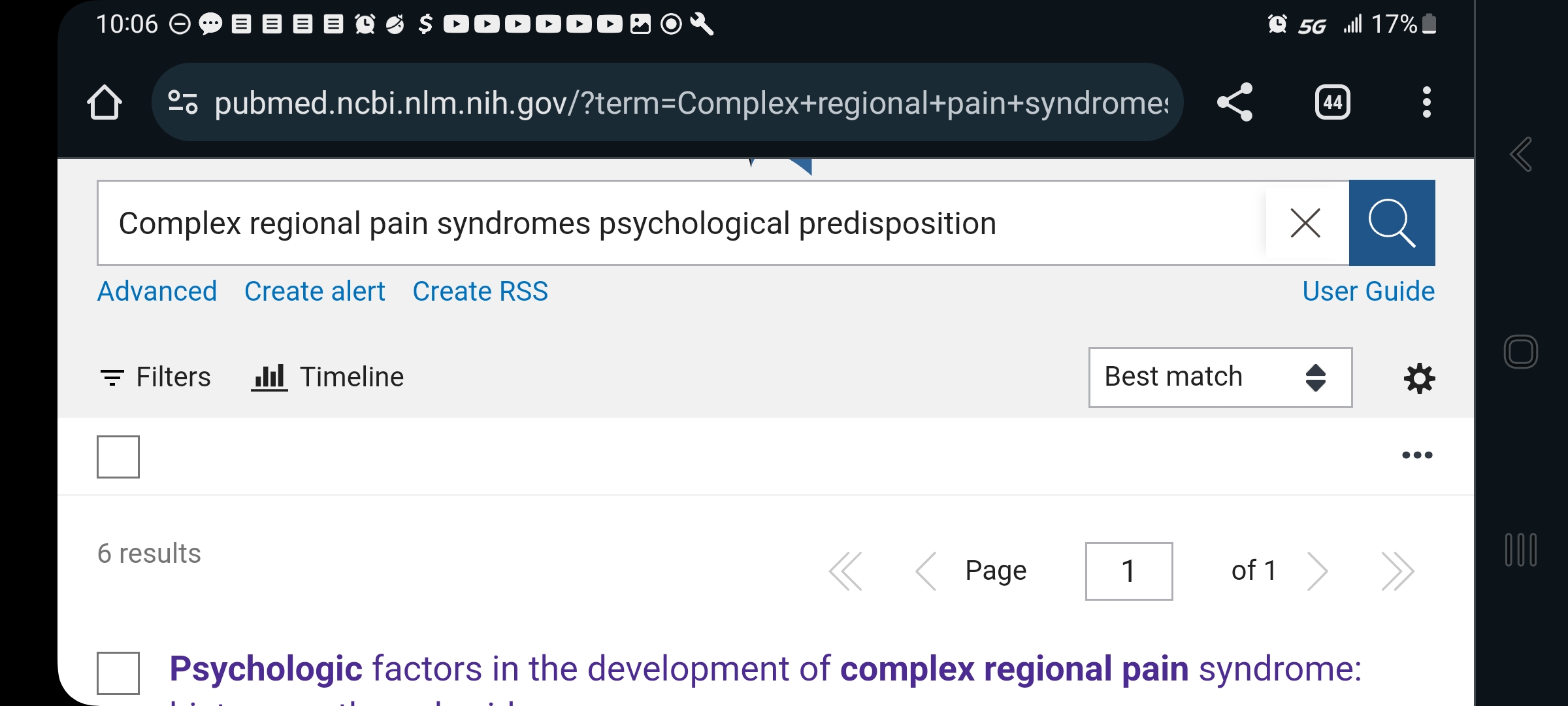
Google pubmed, and you’ll find the National Library of Medicine (NLM) division of the National Institutes of Health (NIH). This is a searchable science library which hosts articles from all around the world, in whatever language they were published in plus English. You can search any valid medical term — for instance, use the full name of your disease rather than its initials, for better results:
Here, you can see that I typed out “complex regional pain syndromes” instead of CRPS.
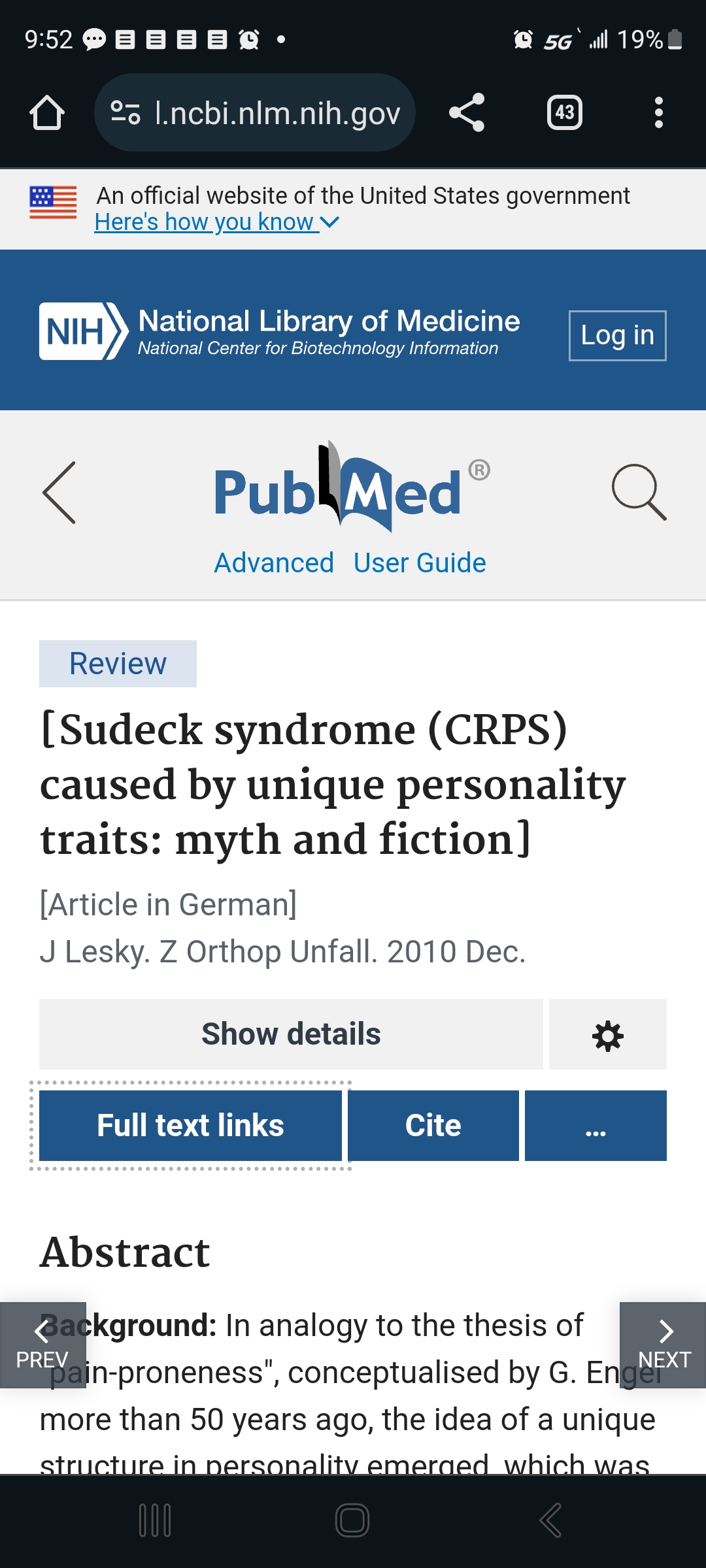
Some of them have full articles that are free to read (look for “Full Text Link”) …
The square brackets around the title tell you it originated in another language. The note under the title tells you which one. Good science is done all over the world. I’m glad we can access so much of it!This image shows what pops up when you touch the Full Text Link button.This is the original site that published this paper. As you can see, it’s in German here, but an English translation is also printed below the German version. For better or worse, English is the world language for science and medicine. I feel lucky being born into an English-speaking family, because it’s tough to learn. All those synonyms… and the crazy spelling!
…But most will show only the abstract, that is, the high-level overview of what the study is about. For our purposes, that’s the most important thing, so it gives you something useful to work with.
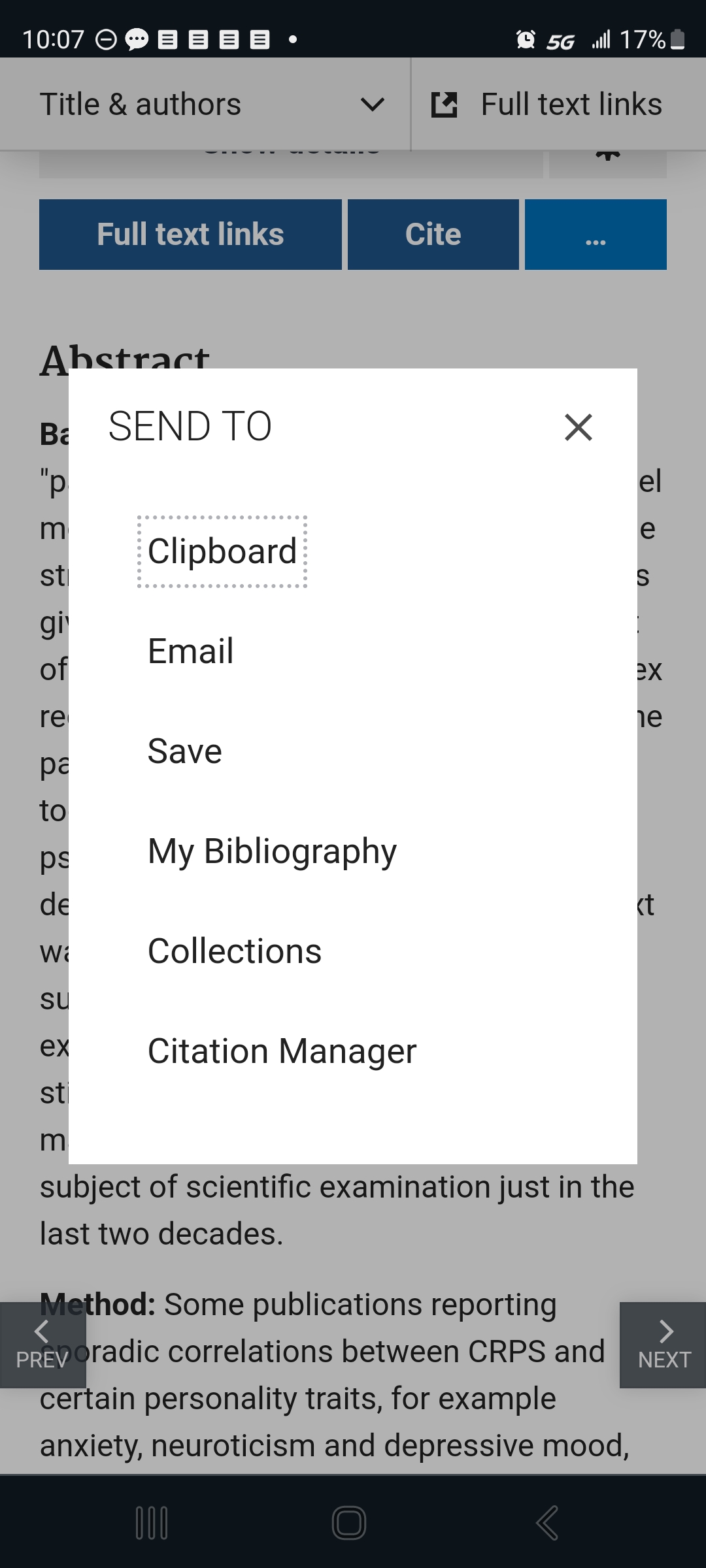
The interface gives you options for saving, sending, and citing the articles.
Touch the “…” button to get this helpful menu. If you get a free account with the NLM, you can use these to help you keep your studies organized and accessible.
To use these, just touch or click the one you want. They do exactly what they say they will.
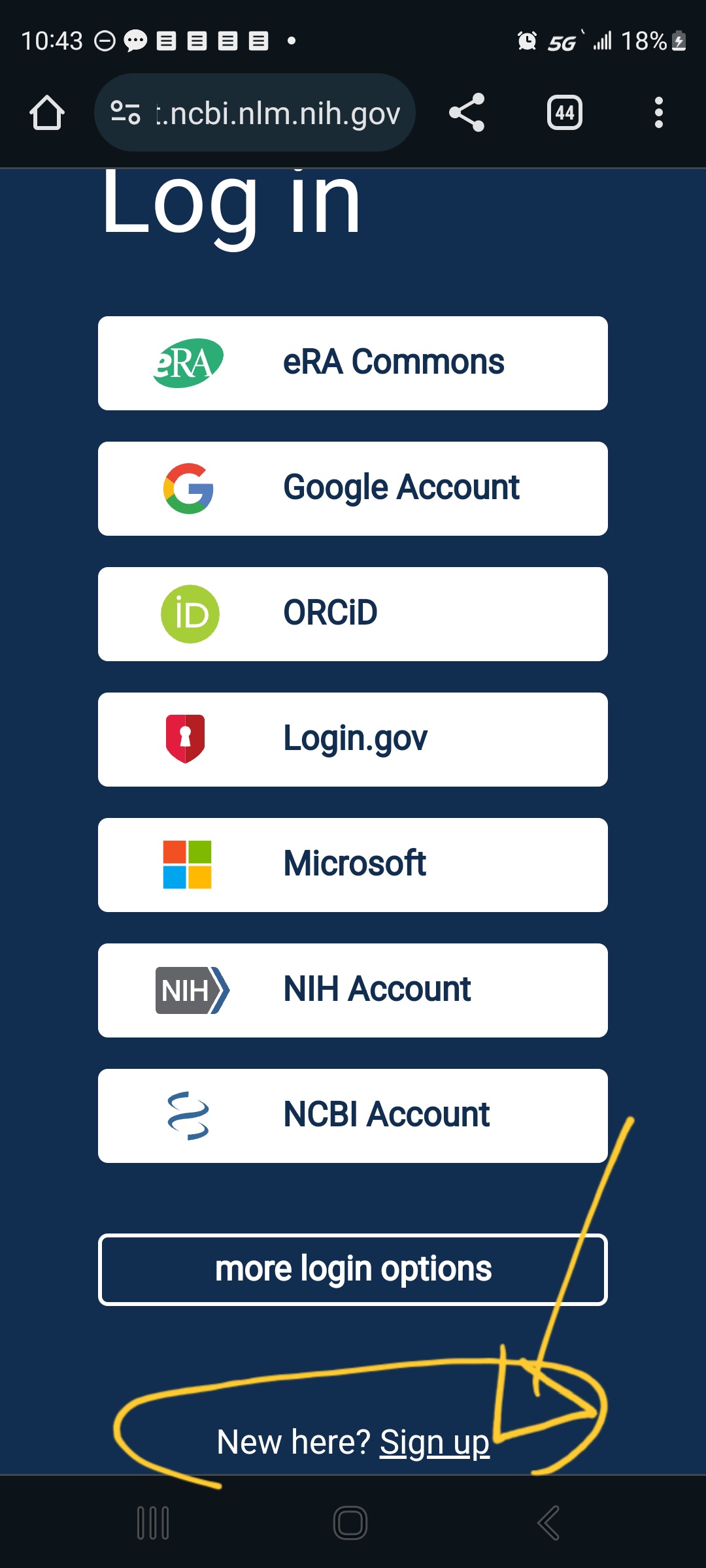
If you touch one of the menu options that requires them to store the info on their side — like “Collections”, “Bibiography”, or “Citation Manager”– it will give you what you need to sign in (if you already have an account) and, at the very bottom, the option to “Sign up”:
The site is very helpful; just slow down and let yourself look at one thing at a time.
Once you feel more self-assured, try out Google Scholar. It’s smaller in some fields and generally less selective, but that can be good. I suggest saving it for later only because it’s got fewer guard-rails. We’re all different, though, and you might find that easier.
These two libraries aren’t identical. They do overlap.
A word about MeSH terms
MeSH stands for Medical Subject Heading. It’s a curated list of specific terms used in the National Institutes of Health materials. This kind of consistency is necessary when organizing a stupendous medical database like the National Library of Medicine.
MeSH terms are listed at the bottom of each article. If that article was useful, you can click the MeSH terms to have them saved to your PubMed search history:
I’ve circled the heading “MeSH Terms”, where it appears below other back-matter after the article.
Here’s a tip: when using their Search tool, don’t worry about capitalization, but be very particular about spaces and punctuation. Copy them exactly.
Using MeSH terms will improve your future searches, because it makes the most of the databases self-referencing mechanisms.
Trust your eyebrows
Best tool in your mental toolbox: when you’re reading sentences you know you do understand and, yet, you feel your eyebrows moving around on your forehead… that logic is not right.
The scientist might be misinformed, biased, pulling a fast one, or just plain wrong, but it doesn’t really matter which — that logic is not right. The underlying pattern-matching part of your brain can tell. That’s a primitive part of the brain and, when you’re paying attention to it, it’s extremely hard to fool!
Trust your eyebrows. If you want to, save the article and come back to it when you know more, so you can figure out where the problem is. I assure you, there is one. Your eyebrows don’t lie.
Feed your brain
Reading science is hard work and brains are big hungry things at the best of times. Feeding it right can be a huge help.
Meds & caffeine
If you’ve got attention problems, adjust your meds and caffeine to give you some extra focus when you’re reading science. It’s a lot more fun that way!
Smart produce
Green, blue, and purple foods are absolutely marvelous for brains — and pain. They feed the nerves, literally. I know you needed an excuse to eat more blackberries, blueberries, collard greens, and rocket salad, aw shucks.
I also know it’s not the cheapest stuff in the market. Explore your local options for farmer’s markets, roadside stands, produce sales, and organized assistance like EBT/food stamps and healthy-living programs giving more access to produce in the state, like they have in Massachusetts and California and other places.
This is a great opportunity to learn more about your condition and to bring what you’ve learned into your life (more on that later), and the upfront effort pays off so much in the end.
Body-safe phenylalanine
Obviously, if you’re prone to phenylketonuria, skip this part! IYK,YK.
Also, keep in mind that this can have an effect on some meds — sometimes giving them a boost, sometimes making things worse. Be sensible, do your due diligence, and study it up for yourself if you’re interested. Also, use your self-documentation skills: note what you do and what it does to you, change what needs to change, and take responsibility for the results of your choices. We are our own best caregivers.
I’m discussing the physiological activity of this thing with the weird name, and what I’ve found in my life and those closest to me. This isn’t any kind of assurance that it’ll do good for anyone else. Put it no further than “hmm, maybe” in your mental filing system and do your own further research to validate what I say and get an idea how it might work for you, yourself.
Basically, phenylalanine is a precursor to the “up” side of the neurotransmitter suite, dopamine and norepinephrine and even epinephrine (they all transform into each other as needed). These neurotransmitters carry messages among the parts of the brain involved in learning and memory. Taking in phenylalanine can have a truly astonishing effect on attention and memory WHEN you’ve got fundamental deficits, as do people with central and longstanding pain and some other conditions.
TL;DR — If it doesn’t make an obvious difference in less than an hour, you don’t need it.
I’ve trialed using aspartame, which went well for me. (Discussing my results with my doctor paved the way to including SNRIs in my med regime, to my considerable benefit.)
Food sources of phenylalanine
This is where hard cheese and smoked or processed meat shine. They’re rich natural sources of phenylalanine. They also have saturated fats which, in moderate doses, seem to help with pain and brain symptoms.
As a moderate part of a well-balanced diet, folks.
This hasn’t been well-studied; it’s one of those things you pick up after being involved with self-managed patients for over 30 years.
It doesn’t take much. I found that 2 or 3 bites of aged cheddar would absolutely light up my brain for 45 min to an hour and a half, depending on my deficit.
One pal of mine keeps meat jerky sticks on hand for study sessions. Aged cheese works better for me; jerky works better for them.
Now, unfortunately, mast cell activation problems have moved cheese and smoked meat out of my diet. When I need a brain boost, and it feels like cheese might help, I have to use a supplement instead.
Supplementing phenylalanine
It’s more measurable to use a supplement called DLPA, or d,l phenylalanine. It’s a blend of natural and manufactured forms of phenylalanine. One works better for pain and another for depression, but the blend seems well-tolerated and helps both. Phenylalanine suppresses certain inflammatory kinases and may help suppress pain at the spinal root (that is, right where the base of the peripheral nerve path comes out of the spine) as well as helping with mentation and cognition. (Sarcastic Sister notes: The recent science about it magically disappeared in the wake of the “war on pain meds” and I won’t pretend to understand why.)
There is a maximum recommended dose before it gets toxic, but if you’re seriously thinking about that, you’ll want to do your own studying, and might want to talk to your doctor about SNRI meds as a possibility. (The N is for norepinephrine, which phenylalanine supports.)
Why bother with learning how to read science?
Knowledge and understanding are the most powerful tools you can have for dealing with complex chronic health problems. It may or may not change what you have to deal with, but it certainly gives you more and wiser options about how to deal with it.
Even if you aren’t ready to start now, you can circle back around to this whenever you want. It’s attainable; you can do it. It’ll always be there (although individual articles and topics may come and go.)
The patients who learn the most and put that to work in their own lives, are the patients who most consistently beat the odds and have the best quality of life over time.
Therefore, better information leads to better living with complex chronic illness. My HIV patients taught me that 32 years ago at my first nursing job, and it’s truer than ever now.
Note: Nobody here says it’s easy. That said, our complex chronically ill lives are never easy.
Pretending that getting through the day is not, itself, almost a superhuman task is a disservice to our strength, so let’s just start off by recognizing that everything we do is really hard work.
Knowing that, I have found that the effort of learning and applying what we learn pays off a whole lot more than passively waiting to be saved and feeling rotten all the while — and still being wrecked & exhausted.
I can whole-heartedly recommend learning and figuring things out. It’s a winner.
My first nursing job was on an HIV unit in 1991. We were in the 2nd wave of the med mixes, so there were some treatment options. We knew which precautions were necessary, and when.
Those precautions had been newly dubbed, “universal precautions”. HIV was the last global pandemic that had a powerful effect on ordinary patient care, legislation, daily activities, travel, everything. The lessons we learned were rolled so thoroughly into our lives that we no longer think about it.
Anecdote from the front lines..
At that time, it was all rather new. Old nurses were afraid to go near any patients on our unit. We had about 80% novice nurses, an unheard-of proportion on a specialty ward in a nationally-ranked hospital in a major city! We had to pay attention, and we had to learn fast.
Because we weren’t abandoned enough already…
Our rather young nursing preceptor had bone cancer in her knee. She went in for surgery as soon as the last of us (me + 1 other) got signed off on training.
But wait, there’s more: as soon as she came out of surgery, she wrote a message insisting they pull the plug on the machines and let her die. Husband supported that, in tears.
Considering how close to hysterical she’d gotten 3 days earlier, when I tried to dig in my heels and tell her I was not ready to practice autonomously and might need more training after her op; and how strenuously this woman — who’d done little but put me down for weeks and express frustration at how slow I was — now insisted I was ready, really ready; and considering how improbable that post-op scenario is, in so many ways… I think she had planned it well in advance. Most expensive euthanasia ever.
Her 2nd-to-last words to me were: “Change your socks. They should be white. Bright colors are not professionally appropriate.” And gave me a fierce look. She came back for a nice goodbye, telling us we were all “good nurses” despite our occasional touches of color (a laugh and a nudge for the main transgressors, me & a fabulous fellow), before she turned and left the unit for the last time.
She’d been working on me about the sock thing for weeks. Slouchy cotton socks in gem-bright colors were still fashionable; drove her crazy.
She was the only one who hated them. The patients, the other nurses, and my immediate supervisor thought my gaudy ankles were delightful. I was referred to as “the one with the socks” and everyone knew. (I also introduced the fanny pack to nursing life. Nobody had heard of it before I showed up with a white, wipe-clean, bleachable one. You’re welcome.)
It’s possible that I got a packet of white socks, as a gesture of respect to that tough young woman… which quickly got grubby-looking, as white socks always do on me, and thus were eliminated from my wardrobe as not being professionally appropriate.
… That was largely irrelevant, but I’ve stopped suppressing my storytelling urge. There are just too many; they leak.
Back to the job of being a complex chronic patient.
It’s surprisingly logical — it just takes a long time to figure it out. I hope this will shorten that course for whoever reads this! There are 3 key principles to follow, and 3 sets of jobs, one for each kind of person involved in each case.
Three key principles
My patients on that ward taught me a lot about how to navigate hard, complex, intransigent illness. There are 3 key principles:
“Grandma was right” kinds of things: fresh air, activity, nutrition, sincere friends, learning all you can — they make a huge difference.
Find the light, or life, in the cracks. Doing #1 makes that a lot easier.
Communicate with others in the way they need to be communicated with.
That can be a tricky one, but I’ve got a lot of material on it. Some of it is here on this blog. And one day I’m going to complete and organize that collection of communication tools. (Any day now…)
Three different sets of jobs
It’s important to remember that you can’t do everything. I learned that (and keep re-learning it) the hard way.
There are specific realms of responsibilities which the important people in this situation have:
My job.
Significant other’s job.
Provider’s job.
They’re perfectly straightforward.
My (the patient’s) job
A note on terminology: some object to the word “patient” as dehumanizing. I’ll let you mull over what it means to think of someone who needs care as less than human. I don’t.
I’m sticking with the word “patient” here, because it describes a person who has specific, unavoidable experiences with alterations in their bodies, care providers, and whatever health-care system they have access to.
Complex chronic patients have a depth and breadth of experience with these things that most people simply can’t imagine — and nor should they. We wouldn’t wish this on anyone.
So, as a patient, my job boils down to this…
Take care of myself; take care of my responsibilities; take care of my relationships. All this includes having fun and seizing little joys!
Manage my illness. This includes: meds, nutrition, activity, learning about the disease and how to manage it, self-care (whatever that turns out to include, but it always includes pacing: alternating activity and rest.)
Track important signs, symptoms, and changes, and document them meaningfully.
Share this info with providers and significant others when it makes sense to.
Find useful ways to communicate with significant others & care providers about changing needs and abilities.
Make all my appointments on time, every time.
Contact my Dr for anything I need their support with: changes, meds, treatments, info.
Get through the days one at a time. (Thinking of the whole span of my existence is not my job. One day at a time is plenty.)
Find life in the cracks: notice the little beauties, regularly do something I enjoy, stop and smell the flowers.
Make time for fun and happiness. It makes me so much stronger!
Be good to my loved ones, whatever that means and within my limits.
Know that I’m the subject matter expert on my body, and hold myself responsible for managing it accordingly.
Significant other’s job
These two principles can be used by people at work, at home, on the playground, wherever. Very simply, “believe me” and “avoid making this harder, whenever possible”.
Believe me
Nobody — trust me, nobody — can make this stuff up, and there are far too many expensively-educated people working on this for it to be imaginary.
If you can’t believe it, then try pretending you do for awhile, just to test the concept, and see how that works.
Learn about the disease. There’s good info out there and I, or my doctor, can help you find it.
If you’re really important to me, come to an office visit with me and ask the doctor your own questions.
Avoid making this harder
Communicate with me about changing levels of activity and needs. I hate to keep saying how broken I am, so let’s come up with a code to pinpoint the different levels of broken that I could be.
Then, I don’t have to talk about how close I am to puking or crying or passing out, you can know anyway, and we can get on with things appropriately.
That’s what I really want — to be as productive as possible for all the time that I can; to be as good a partner/employee/friend/family member as I can.
Provider’s job
Another note on terminology: I’m old enough to remember when physicians, who were relieved that good schools for PAs, NPs, and APNs were starting to flourish, advocated for the term “provider” as a collective noun, encompassing themselves and the advanced-practice professionals who potentiated their work and multiplied their efforts.
That worm has turned, and now it’s not so popular with physicians.
Please allow this old nurse to use the term with all the respect it originally included, in memory of the brilliant and capable physicians who taught me to use it as the inclusive term of choice.
The provider’s job (as of course you know) is threefold: keeping the larger view, providing appropriate care (of course), and providing info and guidance.
This is sometimes easier said than done, because every time I see you is a rough day. You hold more than the power of life or death over me — you hold the power of tolerability or pure Hell. Thus, it’s natural for me to be a little fragile, possibly overwhelmed, in our conversations.
I do my best to be prepared and “keep it together”. I want to make the best use of our time.
Due to the additional insults of pain and CNS dysfunction, I can be subtly or even grossly impaired when I most need to be responsive, intelligent, and clear.
Given all this, please know that your kindness makes a great difference in my life.
Here is what I hope for, from my providers:
Consider context. Notice where I fall in the statistical ranges and how might this affect my care; help me distinguish between reasonable vs. unreasonable efforts, as well as watchable vs. reportable signs/symptoms; steer me through that intersection created by my medical & physiological peculiarities in one axis, and the statistical probabilities generated by reams of studies and years of clinical practice on the axis which crosses it.
Prescribe appropriate tests, ancillary care (physical therapy, occupational therapy, speech therapy, and so on), and medications.
Respond sensibly and kindly to concerns about meds, therapies, and changes in my illness. (Fragile egg here.)
Let me know what I really need to know about my condition, meds, or treatment, before I leave the room (virtual or 3-D), so I neither ignore something important nor over-study and confuse myself. My responsibility to learn benefits from yours to inform me. Also, it helps me to know the right keywords.
Be the subject matter expert on the scientific and clinical knowledge-base for the illness I see you for, and be willing to figure out relevant context that my other conditions create.
See this article about just how fabulous an experience it is to have a physician who does all that. It’s such a relief and such a joy. Thank you from the bottom of my vital signs for doing what you do.
All 3 working together = best possible situation
When complex chronic patients can monitor and communicate effectively, prioritizing our care while keeping life in center stage most of the time; when our loved ones can coordinate around our limits, allowing us to be at our best, considering; and when doctors apply their staggering breadth of knowledge to our particular situations with attention; we have a fabulous chance of doing as well as possible.
I like doing as well as possible. I have a lot to give and I want to be able to give it — that said, my care comes first, last, and always; it’s the only way!
Thanks to significant help and support, good friends and loving family, and some real rock-stars on my medical team, I’m well set right now. I’m almost afraid to admit it, because I don’t want to rock the boat…
And here we are
There you have it: the 3 key principles and the 3 main jobs of living/working with complex chronic illness.
I know they are that fundamental, because I’ve had a few providers almost plead with me to come and participate in their patient support groups, specifically so I could talk about it with other patients.
Well, here we are, sharing this information all over the world! Send this article wherever you see fit. I’d love to know what your support groups think about it.
Patients, caregivers, loved ones of complex chronic patients, doctors, P.A.s, A.P.N.s and N.P.s… feel free to comment. This is about all of us, after all.
In the spirit of this blog’s brief as a “user manual for complex chronic spoonies”, here’s a health update after another interesting year (my personal year starts in May!) with notes on medical support & the relevant self-care for each problem area.
Cultural note:
In American slang, “the Back 40” was (is) probably the least obvious & accessible parcel of a farmer’s land. Either a lot of work or no work happened there, it was hard to find the person doing it, and the effort didn’t show until afterwards.
Good metaphor!
Areas of life…
Mom (& TL;DR): 2+/3, it kinda sucks but I’m getting doctors involved and they’re good. Adjust expectations downward a bit, because this could take awhile to resolve.
Endocrinology
I got a med with a toxic-to-me ingredient (maltodextrin; it’s specifically inappropriate for people with low thyroid!) and that set me back in inflammation, pain, mood, and thyroid function. That’ll take some time to recover from, but…
=> I’m doing All The Things, mostly hydrating & waiting & antioxidants.
Plus a thyroid med I tolerate well.
Not having thyroid supplementation at all for 4 days (after 2.5 weeks of thyroid with toxic crap in it) set my thyroid recovery back further, but let my mood come back closer to baseline and gave me more access to memory & coping skills.
=>More waiting, plus vitamin A, licorice root, and Maine seaweed for the iodine.
And lots of sleeping.
Dr:
I have an appointment with a good endocrinologist in June, which gives me time to look up his articles & see how he thinks, while brushing up on my endocrinology. (Being a passive patient doesn’t work well for me. Too much complexity & too little margin for error. I hope he can cope with a collegially-minded patient.)
G.I.
I tried heirloom corn flour, because I love masa and grits, and the industrial kinds of corn are too hard on me. (Pain, mood disruption, bit more brain fog.)
Well, it took longer than regular commercial corn, and it took making it a staple & eating it a couple times a day, but it turns out that organic heirloom corn can still do that to me. So, more waiting & more hydration, but after Day 2 of No Corn I’m already a little better. Yay!
Good news is, I’ve consistently been able to eat *enough* overall that my body’s starvation response is calming down! I’m no longer gaining weight daily (which is what my body does when it’s starving). I’m able to fit into my biggest clothes that *aren’t* stretchy, another yay.
=> I find that 1200 kcals/day is the functional minimum on any given day. Getting up to 1600 is good, much more stabilizing.
Organic, free-range everything with plenty of olive oil. I have had skillful & compassionate help with cooking since November, and it’s been absolutely life-altering — for the better, which makes a nice change!
Dr:
I’m seeing my GI doc this week. I sure hope he doesn’t retire soon.
Brain & pain
Not so good. It’ll change, but there’s no knowing just when. I’ve got a UI design & documentation project which I badly *want* to do, but I think the better part of wisdom is to write up what my training & experience leads me to envision, and find others to help do the work. Trouble is, when I get to the computer, I don’t want to write it up, I want to just do it… ADHD fail, so far!
CRPS-specific
The bone pain is having a party in my feet, legs, & pelvic girdle. Skin in my arms & legs is more burny, and it’s getting annoying. That feeling of my brain envelope being hot (not something that happens in a normal body) is a frequent occurrence.
=> Eliminating the corn (which spikes up my neuro signalling) and stabilizing my thyroid should help that a lot.
I hope.
Fibro pain
Yeah… May didn’t used to hurt like this. My joints feel like the surfaces do a quick “squish” and ooze steam at every impact.
=>Antioxidants, hydration, pacing, thyroid… and time.
Dr:
I’m seeing my primary on Monday and will ask for a referral to Brigham & Women’s pain clinic to see if we can get a better handle on this.
Ehlers-Danlos Syndrome
Ironically, the more I read about EDS, the more it explains a lot. I haven’t got enough understanding to opine further, but feel free to look it up and put your favorite links in the Comments.
Everything is in a “chase the symptoms” mode until then, and chasing the symptoms means that I don’t get things I otherwise need to manage pain and inflammation, because they trigger spasms and cause tissue tearing, both of which sound like EDS issues.
Welcome to complex chronic illness, where “competing needs” is more than a metaphor — it’s a way of life!
Dr:
I have 2 appointments, one to prep before genetic testing of a more arcane kind than I can get myself, and one to discuss results. The first of these is in November. We made that appointment last fall, so that’s really the best we can do.
Life
Best time of year is here. I hope I can get some recovery & remission, as I usually do in the summer.
The pain & brain fog keep me indoors more than I’d like, especially with the high pollen count making the histamine & inflammation situations worse. (Competing needs again: I love being outside.) It’s just too much to try to mask over all this, and I’d rather not stand out for the wrong reasons. Again.
I’ve been using my rower for exercise, when I can. That’s better for the bone pain than walking on pavement is, and I’m surrounded by pavement.
Major events
Sadly, I just lost an old sailing buddy to his illness.
Worse, I may soon lose a dear & longtime friend to hers, one of my sisterhood which formed around 2010, forged in the fires of the improbable Hell of having CRPS while being intelligent (ding!) female (ding!!) health-industry professionals (ding!!!) seeking effective care for this insane disease (DONNNNNG).
Some things you just get through and hope for the best.
Love makes everything else bearable — and that makes bereavement a stone b*tch.
On the other end of the spectrum of life… my honorary nephew announced I can expect to be a great-aunt this summer, and the first bundle of crocheted baby-gear is in the mail.
His papa, my widowed honorary BIL, is traveling the world with his skills, hard-won insight, and upright down-home charm to spread the word about what *really* constitutes good patient care. The world is becoming better for his work and I couldn’t be happier for him or prouder of his trajectory!
*Huge* yays!
=> I’ve discovered that the way to avoid emotional whiplash is to think about just one thing at a time.
Some of us are *always* living in interesting times.
Conclusion
I’m going to crawl back under my rock & lurk until all this hydration & waiting does some good. Time doesn’t do everything, but it does give other things a chance to work.
Take care of yourselves, and when you can’t do that, take care of each other. (((Hugs))) to those loved ones & spoonie-compatriots who want them.
Many things are coming together and my soul is taking warmth and strength from the concatenation of care. I’m incredibly lucky — even blessed — and I feel my good fortune with all my heart. It’s a great, and unforeseen (by me), turn of events, after decades of raw struggle.
One of these blessings takes the form of a gifted young man who takes my complex & often conflicting dietary needs as a delightful challenge, rather than a terrible curse. His work with me is a hugely encouraging capstone to,
A lifetime of food-nerdery,
A career of nutrition-nerdery (not the same thing),
Decades of increasing dietary stringency,
Years of gastrointestinal fuss.
It turns out that addressing underlying nutritional needs can re-shuffle metabolic activity so that former limits are a lot less limiting.
I know, right? Who knew???
I’ve been dealing firmly with mast cell activation & histamine reactivity, by keeping everything I eat super fresh, freezing it in portions immediately, reheating in the microwave (which tastes a lot better than cooking it in the microwave in the first place), and keeping the dishes & utensils squeaky clean.
After doing this for awhile, it turns out I can eat brassicas again (cauliflower and broccoli, 2 of my favorite veg) without my thyroid flipping me the bird as it passes out.
I feel profoundly rewarded.
Competing needs: no brassicas; lots of winter veg.
Layered needs: calm down the mast cell activity & histamine responses, and my immune system is perfectly happy to take brassicas on board without trashing my thyroid in response!
Also, I was gaining weight rapidly around the time this kitchen-magician showed up; since my diet was so limited at the time (homemade parsley buns, homemade blueberry buns, farm-frozen chicken, and sprouted lentils, with only olive oil & salt for flavoring) it was very easy to do a calorie accounting.
It turned out I was in hardcore starvation mode, getting only 700-1000 kcals/day. That’s not enough. It kicked my cortisol into high gear, which is overdriven anyway due to pain & dysautonomia, and manufactured excess adipose tissue from (apparently) thin air & bad grace.
I’ve roughly doubled that calorie intake; with my kitchen-wizard’s help, I’m getting loads more veg, too, which for me are a sort of cure-all — whatever is wrong with me, it eases up if I get more veg.
Keep in mind that *any* consequence of starvation is unhealthy. Losing 80 pounds to starvation is even more horrifying than gaining them. It hurts less, but it’s more dangerous to kidneys and system function.
It’s a peculiarity of our modern sensibilities that gaining weight due to starvation is absolutely invisible, because being fat is considered so repellent (the word “gross” translates as “fat” — that’s a strong linguistic clue), that shaming & blaming is the default response, even — especially — by physicians who should know better than to disbelieve, shut down, and further humiliate their starving patients.
This obviously needs to change.
My clothes fit more naturally and my feet & legs hurt noticeably less 3 weeks on. So, that’s much better!
Competing needs: more nourishment; fewer calories & more activity, I’m told.
Layered needs: adequate calories, so my cortisol can stop screaming about starvation and let my body work better!
There will probably be a lot more about the details — why are all my veg heavily processed or overcooked? What’s the recipe for those buns? How many diagnoses am I working around, anyway? How do you get onions in when you can’t go near them raw? — but that is, as it were, food for future posts. There’s a lot more info in this topic. It’s possible there are a few books in it.