As the title hints, it’s been another fascinating visit with my pain diagnostician.
His current working diagnosis is fibromyalgia, which he characterizes as being capable of throwing some hairy curve balls (my terminology, not his) including the growing litany of food sensitivities, which solves a major problem in my mind.
Thyroid disease can also trigger the symptom complex that otherwise gets tagged “fibromyalgia” (more on symptom complexes in a minute.) I mentioned that I’ve had my thyroid checked several times and last year came up with Hashimoto’s (meaning my immune system is attacking on my thyroid.) Since I developed the first symptoms of this central sensitization around 16 years ago, it seems not like a precipitating event; since “normal” thyroid activity is not the most meaningful term, I’m not sure it’s irrelevant. I guess I’ll learn more as we go on.
He’s also checking my hemoglobin A1c to check for underlying blood sugar instability. I’m always happy to check that. Also B12 (pernicious anemia etc.) and D3.
Now we come to the fascinating (and crucial) distinction between a symptom complex and a disease. Both are used as diagnoses, but they mean different things. (Yes, I’ve used the word “disease” indescriminately here, for simplicity.) Medically speaking, a disease has a cause that can be targeted, what you might call a diagnostic end-point. A symptom complex doesn’t have that level of targeted responsibility for the illness; it’s a consistent set of symptoms that cluster together often enough to get a diagnostic label, which takes some doing.
Here are the two scenarios.
On the one hand, you’ve got someone with a lot of pain, funky guts, sensory reactivity, and normal labs. The doctor (we hope) rules out any other possible cause, and decides the diagnosis is, say, Fibromyalgia. This is a symptom complex, because it’s described in terms of what it does to the person, not in terms of specific pathogens or organs as the causative thingy. (I’m tired; thingy will do.)
On the other, you’ve got someone with a lot of pain, funky guts, sensory reactivity, and thyroid labs that are out of whack. Further examination of the thyroid discovers specific thyroid abnormalities which can be treated. With treatment, the symptoms subside or even disappear. The diagnosis is the disease of hypothyroidism, with a diagnostic end-point in an organ (as in this case) or pathogen.
CRPS/RSD, Fibromyalgia, and some other hideous conditions are symptom complexes. This is used by some as a reason not to “believe in” those conditions, because they aren’t “real.” This is intellectually dishonest, but it does no good to tell them that; assuming that a lack of diagnostic end-point equals lack of ill-health is blatantly absurd, but this is a reality we must contend with. It’s a drawback of having such a flexible language as English, where the same word can mean different things from one context to the next: in Plain English, disease and illness are interchangeable, but in Medical Jargon, they’re definitely different: disease means specific diagnostic end-point, illness tends to suggest a pathogen, and condition is the catch-all term — but is used more for things that really aren’t diseases or illnesses. Another example on a hot issue: in medicine, narcotic refers specifically to opioid analgesics; in law enforcement, it’s a MUCH wider term, encompassing any substance that legislators have decided is not legal. In courts, the meaning of the term has to change depending on who’s involved, which has to be weird.
No wonder there’s confusion around anything medical. What a setup, eh?
This brings us to the physician ethical structure this doc works with, and where it fits into this patient’s worldview. You can almost hear me purring comfortably from here.
He speaks of himself as a Palliative Care specialist. Most people think of Hospice when they hear palliative care, but it’s wider and simpler than that. It means this physician has chosen a field defined by the fact that his patients will probably never recover. That’s what palliative care means: keeping the patient as comfortable and functional as possible, for the rest of their (probably, but not necessarily, truncated) lives.
Yeah, pretty darn special. How many of you who see pain docs hear them use the term “palliative care” naturally and fluidly, without wincing and scuttling on? It’s a little thing that means a lot. It makes me realize I’m seeing a doctor who CAN be there for the long haul, if need be. Someone who would NOT throw me off with the very natural cringe of frustration and failure most docs feel when they can’t save you, or when you’re in the final downhill slide and they can’t face you dying. He can take that strain without failing me. That’s rare indeed.
Palliative care is the very heart of chronic pain care, and I couldn’t face that myself until today.
So now I just have to die before he retires…
Kidding, Mom!
I’d like to go over his approach more, but the fog is descending; it was an early morning and I’m paying for it as usual. I’ve got lots of notes, though. It’s great food for thought, so, with luck, I’ll come back to it.
My pain diagnostic specialist is elegantly opinionated. Fortunately, he acts out the distinction between being opinionated and being rude about it.
We talked over a few things today. He’s still researching my past exposures to uranium, which he has a hard time believing wouldn’t have lasting effects.
He spent a lot of time combing through the idea that evidence-based medicine (in the sense that doctors use the term, not the sense that insurers do, where it means “how can we treat this as cheaply and barbarically as possible”) is really the best and least scary thing out there. Because, data.
I mentioned Dr. Scott Reuben at this point, and he owned that the scientist-practitioner does have to practice with integrity for the science to be meaningful.
He went on to say that the miracle cases that wind up in the literature leave physicians panting to find the next patient who shows up looking just like that case, so they can try the miracle. Doesn’t happen much, and so, there winds up being a paucity of data on rare cases (like mine) that meets the criteria of medical science as he sees it should be.
In the end, as always happens in conversation with a physician who has intellectual integrity, we found ourselves in the cleft stick of modern science:
While statistical probabilities indicate the best chances of success for groups overall, it has two glaring weaknesses, even in ideal circumstances: statistics depend on copious data, which aren’t always obtainable; and statistics mean nothing in the case of the individual.
Thousands of individuals are studied in order to come up with meaningful statistics. Of those individuals studied, how many respond to the treatment at the level of the group’s statistical probability? How many patients in real life will respond at that level? Pfft. All the statistics do is tell you how much of a crap-shoot a given treatment really is; it doesn’t tell you how well or badly it will do for you.
Last Friday, I saw my allergist/naturopathic MD at Northampton Integrative Wellness. He’s exploring mold toxicity, which sure hits all the hot issues I deal with. It doesn’t meet Dr. Saberski’s mental criteria, as I suspected, but that’s okay — I don’t need Dr. Saberski to follow up on it. I need someone like the docs at Integrative Wellness, who have the relevant background and tools, to follow up on it.
Because of my own experiences, I don’t necessarily assume that a well-educated, well-respected, well-published physician necessarily has a lot of intellectual integrity. However, I’ve come to the conclusion, through our conversations and his decisions along the way, that Dr. Saberski’s entire being (at work) is oriented on intellectual integrity.
We may not view things the same way, and he may not be thrilled at everything I do, but the fact is, he shouldn’t have to be. He’s delighted with my good results when I get them, and if this mold toxicity thing pans out and the treatment goes well, he’ll be truly elated for me — and will keep my chart on file, just in case I come back later.
I find it HUGELY relaxing to have such a resolute scientific conservative with such ferociously diligent, relentlessly inquisitive intelligence, which is completely balanced on intellectual integrity, on my case.
All I have to do in relation to the standard science is let him do his job! I do not have to educate this one — quite the reverse! I savor our conversations and make extensive notes, because he always has something to teach me. (Today’s exciting topics: what makes me NOT look like CRPS; the Flexner Report in history; how anesthesiologists, who have the diagnostic training of a spaniel, wound up running pain clinics — another stupid consequence of US insurance companies; and how the nociceptors and immune signaling in the skin are all entangled into being one thing. Woot! Fun stuff 🙂 )
That, frankly, has been unheard of for most of my time with this illness, whatever it turns out to be. I’m well and truly rid of the fearful weight of using my rare full-brain times to try to stay one step ahead of the risk to my survival and management that every doctor visit can be.
I can use my full- and even three-quarters brain time to study up on the stuff he can’t be interested in. For one thing, the vocabulary and writing style is usually less klunky and demanding. For another, that is supposed to be my job.
Patients should figure out what they can do for themselves without making things worse, so I’m happy to do that.
Now, I’m going to find out more about mold toxicity, methods and treatments, plus what data do exist on what to expect from those treatments and what they do in the body. According to my current info, the main researchers are Shoemaker on one hand, and Nathan and Brewer on the other. My allergy/naturo doc is leaving, so I’ll have to start with another one at the same practice. This means I’d better prepare, so I can move the conversation forward a little faster than usual. That means being able to speak her language in regard to what we’re looking into.
I find it’s best to impress doctors right off and for the first several visits, and then, if I’m having a bad day another time, they have a meaningful bar to measure against, and they don’t lose respect for me or dump me into that “just another whacky pain patient” mental garbage-can. I work hard to make visits as useful as possible, as regular readers know.
I’m also getting ready to do another massage intensive. Looking forward to that! It’s pretty uncomfortable for a couple weeks (arnica pills 6c and 30c, and Advil Liqui-Gels, are essential pre- and post-massage medication), but the payoff could be so spectacular. I’m tired of the downward slide and intend to crank up the functional level one way or another.
Winter bit me pretty hard. It’s time to start biting back.
“Visis mu! I care for you, so let me hand you this wildly inappropriate thing, because I’m too rushed to think things all the way through!”
I have written about dealing with careless, ignorant, detached, and outright bad doctors, which is needful and — given the many problematic layers of living with chronic, intransigent pain — appropriate. However, I’m also a nurse, and I really do see things from both sides.
You’re both right.
Having said that, I normally have to pull for the patients, because only one person in that exam room is definitely NOT paid to be there and is NOT on duty, and it’s the one seeking care.
Patients
Patients need more advocacy, partly because few of us have the vocabulary to make our real needs and issues understood, and partly because the mere label “patient” instantly drops a person out of the realm of “real human being” in the minds of providers. If you’ve ever seen, or been, a doctor or nurse who needs medical or surgical care, you know darn well how your erstwhile colleagues speak to you differently from how they did before — but still more humanely than they do to most other “patients.”
Being labeled a “patient” is damning. You become a thing, a self-steering talking object, with only a surface resemblance to “real” people. Your main appearance in the eyes of the system, and, at some level, of those who work in it, is as a collection of problems. Your main purpose is to respond to treatment and go away cured.
Chronic intractable pain syndromes become zero-sum games from this standpoint, because pain is inherently demanding — even thinking about pain is painful!*1 — and managing these disease states rarely involves being able to “go away cured.” So, from this institutionalized standpoint, chronic pain patients are set up as failures from the start, because we can’t do our job — go away cured.
Explains a lot, doesn’t it! This unfortunate fact is simply one more thing to work around.
Those of us with intransigent pain syndromes are lucky in one respect — we have interesting sets of problems, and intelligent doctors find that intriguing! Appealing to their curiosity is often more effective than appealing to their humanity, because it gets them where they work best.
A nurse who’s a patient
It has taken many years of painfully humiliating introspection for me to come to terms with this basic dehumanization of patienthood. I was a good, solid, compassionate nurse, but I did not treat people who came under my care the way I would have treated my friends or relatives if they were in my care.
Many reasons for that. For one thing, the profit-driven scheduling doesn’t allow time for anything more than slinging meds and essential care; spending too much time with one patient means putting other patients at risk.
Beyond that, there’s a primal survival reflex involved, because there are things nurses have to do for patients that would be unbearable to do to a friend or relative.
We have to do all of them, thoroughly and without flinching, because they need doing in order for that patient to heal; and we still must be able to come back to work the next day. So, we create a little distance that we can do the work from.
They’re all looking at you pretty much the same way. Lovely, isn’t it?
Patients are Other. When they become too human, they can quickly become embarrassing, and every human on earth cringes away from what’s embarrassing. (Just as every human on earth cringes away from what’s painful, and this explains why we tend to get abandoned by our friends and by the system when our pain becomes too obvious for them to bear. That, in turn, is why we get so crazy-good at minimizing the appearance of being in pain; we don’t like the abandonment, and we don’t want to hurt those around us anyway.)
Speaking as a patient and long-term survivor, starting from the underdog position is a terrible position to negotiate your ongoing survival from.
So, I spend most of my time advocating for and educating my fellow patients. They’re the ones who need it most.
However, once in awhile, something hits me, and I feel a point needs to be made.
Doctors (and other care providers)
This article is a good little anecdote from the ER, my old base:
And that, right there, is the juggling-act providers have to do. The decent ones, which is most of them (really), put their hearts on the line every day, knowing they’re imperfect and doing their best anyway.
When I was doing something intense, like dressing a complex wound or teaching someone about their disease or (obviously) coding someone, that patient was the most important person in my life. I threw everything I had, with all the control and skill I had, into the moment-by-moment demands of their care, the whole time that they needed me.
That patient was my life.
Then, whether they lived or died, I had to arrange what happened next, clean up the mess, and leave the bedside, only to go to the bedside of someone who needed me perhaps just as badly in a wholly different way.
No matter what had just happened, after all that effort and dedication, I had to leave it behind and be ready and focused to correctly identify and move forward with the next patient’s tasks.
So, yes, I rarely came off as a fluffy cuddle-bear (which I tend to do at home), and a lot of my responses could be pretty formulaic, but when the chips were down, “he [still] wasn’t my child.” He, or she, or they, was my whole world.
Being able to turn away from that intensity is what makes it possible to turn back to it at need. That’s a tough thing to deal with when you’re on the wrong end of it, when you’re not the one dying on the table or getting your insides pulled about. You know you matter, and want to be treated as if you do. That’s right and proper. It might be too much to ask of a full-time RN. (There is definitely something weird about that.)
Nurses are the bedside providers. Physicians are the directors of care, deciding who goes where and why. They’re accustomed to deciding what happens, and expecting others to make it so, so that the patient can get better and go home.
Chronic care is always a long game, sometimes a waiting game, and doctors are dealing with people who simply can’t do what the doctor’s expensive education said was the doctor’s job: “send them away cured.” This means that the chronic care provider is also set up as a failure from the start, as some have found the grace and integrity to express. *2
This must be a special kind of tricky to learn to deal with, so it doesn’t surprise me that not many otherwise good-hearted people, who go into medicine for laudable reasons, don’t always manage it with the tact and decency that chronic patients (rightly) expect.
In that case, it’s not a bad idea to find a way to waft this article their way… It’s not judgmental, and it provides much food for thought, for physicians and patients alike:
As a side-note, one strategy I find useful for getting through the thing-ness of being a collection of probl– er, a patient, is being as pleasant and amusing as possible. This creates a safe-zone of humor while drawing the provider in past the boundary of “thing-ness” I’m reflexively put in. The wry, black-nailed, hangman’s humor of living with something so vile and refusing to let it win, coming out in my burbling and whimsical-sounding tones, is probably sufficiently unexpected to blow categories out for the moment anyway.
If I can make them laugh with me (while checking me out with a puzzled “are you serious?” kind of glance) I’m halfway to being human in their eyes, and still being treatable. Then, I just keep up with my due diligence (timelines of care, understanding my treatment options, studying up on things we’ve discussed, etc.) and — with the exception of one doctor out of two dozen, who I thought was a buffoon in any case — my relationships with my doctors have been remarkably good.
*2: A particularly dazzling piece from a UK doctor on coming to terms with treating (and living with) chronic pain patients: https://abetternhs.net/2013/09/07/pain/
This is from one of my Isypedia-type replies to someone with a dreadful case of clostridium difficile (commonly known as c.diff) who had been told to use antibacterial soap to wash.
NB: This is not an opportunity to argue about antibacterial soap, but a sharing of experience from someone who was on the front lines of the “soap revolution” over a quarter of a century ago.
///
A word from an old nurse on this question, one with leaky gut, bouts of multi-system candidiasis, and assorted other gut issues, as well as c. diff …
About c. diff
C. diff is common in hospitals and is an opportunistic infection. (Doctors carry it from bed to bed on their white coats, and few of them even wash the darn things more than once a month. This is disgusting.) Once it’s in you, it hibernates, and comes out in flares periodically, usually when you’re stressed out or when your immune system is down. There’s no question of curing it, but of suppressing it and managing outbreaks.
Healthy gut flora are the first, best line of defense. They simply crowd it out and leave no room for it to grow. A normally healthy person might do fine with eating yogurt, but those of us with chronic or profound illnesses usually can’t meet their needs this way. We need the big guns because our gut flora are likely to be very weak,very few, or both.
There are some great probiotics out there. Good brands are pretty numerous. They include Jarrow, Garden of Life/RAW Vitamin Code (my personal favorite), and Ortho Molecular Products. I use the RAW Vitamin Code 5-day Intensive product for 2 weeks at a time, when I need to reboot my gut. Recently, I had candidiasis and c.diff flare up simultaneously, so I’m using the Ortho Molecular Pro Biotic 225 (tastes weird, so I mix with juice to cut the funk) for 2 weeks and then I’ll do a round of the RAW Intensive (which has a much broader spectrum of organisms, something my body really needs for maintenance — the longer a person has CRPS, the fewer gut species that person has, oddly enough) for 10 days or so.
I get these products on Amazon or at Vitacost.com, where they can usually be found at near-wholesale prices.
About the social and practical aspects of soap
Men have trouble with soap. (I’ve had to teach males of every age to wash their hands for dressing changes or eye care, so yes, I can confirm it absolutely.)
It doesn’t mean they aren’t capable of using it well, any more than women are incapable of lifting weights; they just have to put a little more effort into it, but almost all of them are capable of becoming very capable.
No, really, it’s true. They can. They just have to put a bit more work into it.
Where possible, many men would much rather have a toxin or tool to do the cleaning job for them — hence sonic cleaners and autoclaves for equipment, and benzalkonium chloride or alcohol cleaners for the skin of male responders and providers.
These aren’t as good as soap and water. Notably, alcohol cleaners, which are widely used in hospitals and do kill many germs, don’t even touch c.diff — a peculiarly hospital-based pathogen.
These products are considered good enough, and are certainly a great deal better than nothing at all.
If men (at least, US men) have to use soap, though, it seems easier for them to think about if it’s a tool-ish sort of soap — Gojo (by every mechanic’s sink, next to a fossilized bar), Lava soap (which feels like dirt and has powdered rocks in it), or antibacterial soap (which sounds medical, and therefore like a specialized tool.)
That’s a lot of needless expense. Also, and more importantly for the purposes of this blog, it’s becoming clearer that there are toxicity issues with antibacterial soaps which affect men as much as women and children.
How to clean your skin so well at home, only a surgical scrub could be better
Whatever body part you’re washing, whether it’s hands or what the medical profession delicately refers to as the “peri area” (Latinists, look away from that) and what most Americans call “the crotch”, there is a very simple way to get as clean as you can, short of a surgical prep.
Here’s the magic:
20 seconds by the clock(you’d be amazed how long that really is) with regular hand or body soap,
On your hands, from nails to wrist; Between your legs, from front to back; In both cases, right through all the crevices and any wobbly bits,
Then rinsing well afterwards,
This process will get you as clean as, or cleaner than, any amount of antibacterial soap, without the side effects. That’s what the independent science says, over and over, plain and simple.
The problem is, of course, that most people (especially men) have trouble spending that much time with soap and water.
Personally, I do a quick pass with soap to get the worst of the stinkies off, and then do a second and sometimes a third pass, front to back. I do this every time I shower, and when I’m too sick to shower but can still stand up at the sink to wash. It adds up to 20 seconds, usually closer to 30. My nurse’s nose finds my sick-body smells distressing, so I like to clean them off completely.
When I’m really not up to washing well for at least 5 days out of the week, that’s when the troubles start. Usually, diet and hygiene keeps my gut content, but I recently got a virus and then a long pain-flare and that put me down for over a week of very little proper washing — plus, of course, diminished immunity. That’s probably what led to the multiple gut flares. (They’re much better now, thank you.)
Making the right choice for you
Bottom line is this… IF you can trust yourself to really clean yourself properly, which means 20 seconds of soap (in 1, 2, or 3 increments at a time, as long as it’s 20 seconds total), then ordinary, nontoxic soap is just fine.
If you can’t trust yourself to do that, then yes, you need the extra killing effect that the antibiotic soap can have on pathogens, and will have to risk the consequences.
For triclosan and its relatives, this includes muscle wasting, dose-dependent (the more you use it, the worse it gets); for most others, it includes moodiness, suppressed immunity, more skin issues, and all the stuff that goes with endocrine disruption — possible neurological issues like pins-&-needles and faulty neuro, endocrine, and hormonal responses. (You have to watch the medical science closely to find some of those things, because they rarely make it into the mainstream press. Bad for business.)
And that, ladies and germymen, is the lowdown on how to choose soap.
I’m going through one of those periods where I’m just tired of my body hurting.
This is one of those offhand remarks that makes fellow painiacs nod understandingly, offer a kind look or emoji, and move on, but it makes normal (-ish) people with good social skills cringe and stops the conversation in its tracks.
I don’t want to make nice people cringe, and I don’t want to kill the conversation. I was recently reminded how hard it can be to avoid that while answering “how are you/what have you been doing” with any honesty. In fact, I find myself talking about most of the past 20 years in terms of not getting dead.
I think that’s a hoot, because it’s so improbable and so much against my initial setup and programming. (I have a truly dreadful hangman’s humor.)
Needless to say, most people think it just sounds grim.
My setup and programming
I’m the offspring of a diplomat and a working artist, well-traveled and extremely well-educated, Seven Sisters undergrad… until I went off-road and became something totally bourgeois and practical (a registered nurse) and, when my immune system conked out for no apparent reason, went on to become something nouveau and nerdy (a writer documenting high-end programming software.)
It was a sweet setup: good brain, strong body, great start to a useful life, good plan B when plan A failed.
Eventually, this promising start led (via surgical complications, neurological disruption, extensive worker’s comp and SSDI abuses, failures of care and denials of treatment, tediously protracted near-death experiences — a term I’m longing to refine — and years so close to utter destitution I refused to look at dumpsters because I knew I was not far from winding up in 2 or 3 of them simultaneously, like the other invisibly disabled woman of my age, build, and coloring who landed on the streets of Oakland) to my utter destruction as a professional entity.
That was definitely not in any of the scripts my life was supposed to follow!
My childhood friends now have their own businesses, pocket palaces, successful careers in the arts (most), policy/diplomacy/public service (some), and STEM (a few), and in raising children with little concern for whether they can feed them. I’m deeply relieved and happy for them, while realizing that my own life-path got so completely hijacked I have no idea what I’d be doing if it hadn’t been for this.
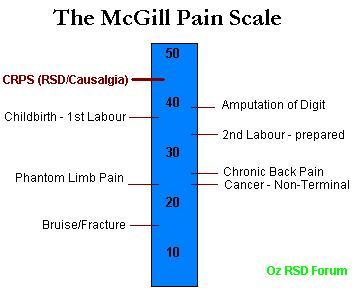
I bet I’d be complaining more, but I’d be doing more too. I wouldn’t be hurting this much for decades, if ever, and even then, only if I had terminal cancer.
Terminal cancer can be a 50. Image from the Australian RSD syndrome support group, Oz RSD Forum
Which brings us to a key point: to discriminate against the disabled is to discriminate against your future self. We’re all getting older; with more lifespan come more proofs of mortality, which include reductions of function, stamina, mobility, and even memory and reasoning.
These, folks, are disabilities, and either they will happen to you or you will be a premature death statistic. There’s no third option.
This is why, when you discriminate against the disabled, you discriminate against your future self — and all those you love.
I wish legislators had the humility to remember that. Perhaps you’ll remind them… Find yours at www.usa.gov.
Where was I? Oh yes.
Pathetic? No.
How do I talk about the last 20 years, especially the last 15, with a person who hasn’t spent an appreciable part of life dancing with Death and occasionally taking the lead?
She looks more embarrassed than anything. Makes sense to me.. From openclipart.org.
How can I convey how incredibly marvelous it is to have a minimum of 2 functional hours — consecutive hours! That’s thrilling! — nearly every single day? And yet, I used to work 10 or 12 hours at at time for preference because I loved immersing myself in the work.
In comparison to that, isn’t 2 hours pathetic? Especially because I did very demanding work, and 2 hours of noodling around in the yard or walking around downtown really doesn’t compare.
It makes me realize how long it’s been since I even thought about the razor-wire-bound memories of “how I used to be” and “what I used to do.”
I compare only as far back to 2008-2012, the pit of the pit, the nadir of my existence.
Bosch knew.
Compared to that, I’m fantastic! Being fantastic is a great thought!
Being at maybe 10% of my youthful vigor is actually amazing, because during that time, I went from being so close to dead it took 25 to 30 minutes to drag myself, fist over fist, all 6 feet from my bed to the other end of the settee, to feed the cat in the morning. I think that level of function (or nonfunction) is a percentage of my youthful vigor that’s several digits to the right of the decimal. It felt like a negative number, that’s all I can say for sure.
There’s nothing I can do about the past, only the future. That’s not pathetic, it’s just life.
Actually, I feel that way about most of this chronic-illness gig. It’s not pathetic, it’s just life.
The power of “use it or lose it” as a tool under your control
The trick to living with chronic illness is twofold:
Figure out what it takes to manage your illness without letting it take up all your focus. It does not belong in center stage, or not often anyway. Life belongs in center stage. Figure out how to make it so.
Figure out how to have a routine, some sort of rational approach to every day. It’s all too easy to lie back and let the world go by. Speaking as an old nurse, I know the immovable truth of the old adage, “use it or lose it.” Having a routine stabilizes the body’s coping mechanisms; knowing what to expect soothes the central nervous system and simplifies healing. So, make a routine; decide what happens next. Make yourself do things, alternating activity and rest. Use your body, use your mind, rest, then use different aspects of your body, different aspects of your mind, rest, and so on.
These two strategies allow me to make more room, more time, and have more attention, for joy.
Joy is not a luxury; it’s essential to proper function.
The gut, brain, immunity, everything, are worse off when there is no room for joy. Whether I can appreciate my partner, the sunshine, a lolcat, whatever, I grab each opportunity for a shot of delight. I call those bursts of joy “brain juice”, because they boost useful neurotransmitter patterns and, cumulatively, reduce my pain and improve my function.
Bit by bit, even as age creeps up and new issues arise, I find myself better and better able to make use of what I still have. In fact, over the last year, with safety and sanity finally framing my existence, I’ve regained an amazing amount of function. I’m so pleased! (Oo! More brain juice!)
I still don’t know how to explain this to a normally healthy person without sounding like something from another realm of existence.
Different is probably fine
Perhaps I am from another realm of existence.
I’m certainly from another realm of experience; longstanding profound illness is special like that.
Perhaps I simply need to get over this idea that, just because I’m back home or just because I’m talking to someone who knew me when I was an arrogant young jerk and saw beyond that to someone worth liking, I should fit in with them.
Perhaps I should have more faith in myself to be interesting and likeable enough to shine through even the CRPS. I clearly shone through the old arrogance and jerkiness, somehow.
I’m far less confident, eloquent (in person), and humorous — at least, less intentionally humorous — than I was in my 20s or 30s, but I’m a whole lot more confident, eloquent, and (occasionally intentionally) humorous than I was a few years ago.
So, I need to remember to keep my focus relevant, and not think too far back.
Emotional boundaries: My pain shouldn’t be your pain
There’s a trick to disclosing without wounding, even when what you’re disclosing is tremendously difficult. Good boundaries are key.
You may have noticed… people tend to pull away from pain. It’s an ancient reaction that happens in the most primitive parts of our central nervous systems. That means, when we’re too raw about our pain, others may pull away from us because that primitive response combines with their emotions around pain, and our pain makes them hurt emotionally.
I remember how I used to open with the idea that my pain is my pain and others don’t need to imagine it or take it on.
We each have our own load. I’ll keep mine; it’s my job.
This approach of “it’s not your pain, so let it go” frees many people up to re-engage from a rational distance which works for both of us. It’s important to give others the distance they need, because then they don’t feel a need to pull back further to protect themselves, and can stay in contact. They don’t feel driven to pull away from all that pain.
Each of us, well or ill, has to carry our own load, and really isn’t equipped to take on others’ loads as well. I try to remember that and respect the loads of others. It usually works out well.
Come to think of it, it’s essential to relationship maintenance.
Taking it on vs. bearing witness
When I was a nurse, I dealt with harrowing human experiences all the time. I could handle it with real care, and go back next day and do it all again, because I was clear that my load was my load and their load was their load, and the most healing and empowering thing to do for another person is to bear witness to their struggle without trying to take over. The one with the struggle is the one best qualified to find their best solutions; having that implicit faith in them, I found, is tremendously powerful.
For those of us in dreadful situations, we don’t get to choose the reaction others have to our struggles. All we can do is try to back-lead, essentially, guiding them tactfully to a more comfortable position.
Allowing well-intended people to bear witness in a safe way is a natural outlet for the sympathy and compassion evoked in decent people. Letting them get sucked into the awfulness doesn’t help anyone.
Put that way, it’s a lot more clear to me. It’s another form of radical presence/radical acceptance, a mental tool which boils down to, “Things may suck right now, but here I am, it is what it is, and this will pass.” Try it — you’ll be amazed how much mental energy it frees up.
The approach for discussing my illness with others may go more like, “It sucked then and it sucks now, but the worst suckage is behind me, it gave me great opportunities for growth and I took ’em. At this point, I’m better at looking ahead than looking behind, and hey, I’ve got interesting projects going…”
So, first I should clarify the needful boundary between my personal load and the rest of the world, and then I can discuss all this with some detachment from the gluey-ness of remembered distress, unbelievable losses, and intransigent pain, and best of all I can point the conversation towards something much more positive.
I’m still not sure exactly how to do that, but I’ll practice.
Well, I don’t know about you, but I feel a lot better about this already. I’m grateful for your company as I figure out my rubric for yet another tricky twist of the Rubik’s cube of life.
I take good care of my brain. I work hard at learning more all the time about how to support and foster it in spite of this tedious collage of illnesses. Neurology interests me — always has. Now that it’s so personal an issue, it’s positively compelling. Neurology’s very complex, and hooks into everything — fascinatingly fractal, in the way it repeats the same physiological “phrases” to very different effect in different parts of the body in response to different changes.
I’ve been wrestling with my gut this past year or so. Lately, it looks and feels like someone’s taking a bicycle pump to it and bringing it up a little more every day. When it interferes with your breathing, that’s a lot of bloat!
I’ve found the gastrointestinal (GI) system to be a bit of a trial. It’s very complex, and hooks into everything. There’s no getting away from the endless iterations of its main roles of sensing, transforming, processing, and discarding: at the intracellular level, intercellular level, endocrine level, organ level, and so on.
Some observant part of my brain notes that the same characteristics I find appealing in neurology, are the same ones I find appalling in gastroenterology.
And the gut has so much STUFF in it…
The liver parked under the ribs at one side, the spleen at the other, holding half your blood at any one time, right across the top of your abdomen;
The endless loops of squirming intestine, stretching and shifting within their blobby webs of mesentery, shoving along several pounds of food residue at any one time along its length;
Lymphatic nodes linked in constellations in the shining webs of mesentery and glistening loops of intestine, ready to respond instantly to allergens or pathogens or anything else in your GI tract that could make your body revolt;
Major vessels, the abdominal aorta and the vena cava, coursing alongside the spine, apparently apart from the mess, but branching out so thoroughly and so minutely into the organs and the mesentery that the smartest rats in science couldn’t make it through that maze;
The tenth cranial nerve, forming an intimate and instant link between your brain and your gut, linking your brain directly to the largest grouping of nerves outside your brain, the nerves that surround and penetrate your organs and your gut, embedded in and supported by that amazing net of connective and fatty tissue, the mesentery;
And let’s not even go into the endocrine system, responding minutely — at the level of individual molecules at times — to the constituents in your food, the way you feel about them, what you need them for right then, what else you’re sensing at the time, and even what time of day or year or month it is… then hooking the info back out through the nervous system, cardiovascular system, lymphatic system, and of course the gastrointestinal system.
I was sitting in my Epsom bath today, mulling this over after the battery in my e-book died. I had done the squishing of my legs and arms with the washcloth, and ran it over my neck and back and sides too, but had a terrible time making myself touch my abdomen. It felt just awful. It also felt like it was somewhat detached from me, like it was floating a couple of inches off my back and spine, simply hovering, slightly displaced, in front of the rest of my physical self. Touching it was deeply upsetting in some way, triggering a wordless revulsion.
This is not an unusual experience for CRPSers. We often feel as if the affected parts of our bodies are almost separate from us, or like they belong to someone else, and touching them is — even apart from the allodynia — a crankiness-inducing, unpleasant experience. It’s a perceptual trick the brain plays, probably part of its general effort to manage more ghastliness than it’s really set up to deal with.
One reason I do the Epsom baths (and the stretching, and the activity, and the relaxation meditations, and the aikido/tai chi/qigong, etc.) is to stay on good terms with my body. That whole self-alienation thing is just too wrong, to me — my life is always best when I’m in my skin, so to speak, whether or not my circumstances suck.
Also, to be fair, my body has done nothing wrong; it just got some of the shortest darn straws out there, and it’s doing its mighty best to manage that. It doesn’t deserve my loathing at all. So, I work to keep on good terms with it.
This is probably one reason why I’m still often functional, frequently productive, and can still walk a mile without sitting down to rest on a good day — even after 15 years with this disease on little or no medication (here’s why no CNS depressants like narcotics, here’s why minimal other meds.)
Anyway, there I was in the bath, watching my belly inflate and almost float away, even though I was Epsom bathing (which usually calms my systems down), and realizing I was finding it unbearable to touch the darn thing, even though it was practically in front of me.
I thought, “Neurology is not that hard for me. Why is gastroenterology so impenetrable? Why am I making so little headway on figuring out this stomach stuff, and dealing with so many setbacks? Why do I get these little tailspins of terror about it? What’s going on in… the second largest collection of nerves outside my brain?” I said, as the lightbulb over my head turned on.
I thought, “I’ve been having a lot of trouble with gastroenterology. But I can usually do neurology.”
And the word for the neurology of the gut, ladies and gentlemen, is neurogastroenterology. (Break it down: neuro meaning nerves, gastro meaning stomach, entero meaning inestines, ology meaning study of. Now you have it.)
I’m pretty sure I can do that. I can sure take a stab at it.
First lesson: review the vagus, a.k.a. Cranial Nerve X. It’s a doozy.
It’s been a crazy winter, even for New England. Those of you with pain syndromes know what that means: changeful weather means unstable pain neurology which means more pain and less brain.
I’m so much more stable here in other ways that I found it frustrating to be soooooo daffy. I wanted to tuck that daffiness back behind the dam I can usually hide it behind, and use the creative and practical components of my mind to drive what I show in public.
I revised my supplements a few times, and finally found a routine that does seem to stabilize things a bit better, although it’s kind of hard to tell (it’s like inspecting a crystal with the lens inside, or possibly the other way around.) I’ve stopped fiddling, and will let the test of time tell me how this regime really does.
Also, we’ve had 2 or 3 strains of flu (so far) dancing through the household. The second one was nice, because the really awful part lasted about 5 days and it had an incubation period of about 6-7, and we got it one by one; as soon as 1 person got really sick there were 2 people to take care of him or her. In one case, this meant miso and ginger soup; in another, raw garlic in mashed potatoes; in a third, goldenseal and vitamin C; in all cases, loads of homemade chicken soup and buckets of fluids.
I’m not sick of homemade chicken soup, as every pot is different, but I am *so over* herbal tea, broth, diluted juice… everything. I had a big mug of plain hot water yesterday because at least I’m not sick of it.
I find that viruses affect my brain. They have for as long as I can remember. One of the first signs of viral illness, for me, is getting cranky and forgetful all of a sudden. With all these brain issues I have now, it just turns the volume of pain, reactivity, and goofiness up to 11.
Into this brew of brainlessness, add one more element of confusion: my most expensive brain prescription, Savella, looks exactly like my cheap antihistamine, generic Zyrtec; I take them both twice daily.
You can see this coming, can’t you…
I found out a week ago that I’ve been double-dosing on Savella and underdosing on Zyrtec. (No wonder my asthma has been acting up.) That, more than the virus and sinus activity, would explain the intense dizzy spells, disembodied feelings, uncharacteristic irritability, and eerie emotional detachment from my nearest and dearest. (No medication is harmless. Now you know what an overdose of SNRI does to me.) It was a relief to know what really caused all that, but it still sucked to go through it.
So, thanks to the daffy-dam getting burst by those bugs, I blew my brain out of the water (and also blew about $150!) AND set myself and my housemates up for a few weeks of needless unpleasantness. I’m still recovering, but well enough to think coherently about it, so that’s a huge improvement.
To my morning pre-pill routine of apple (malic acid) and sunflower butter (digestible folate, minerals and anti-inflammatory oil), I now have ~1/2 cup of defrosted Boreal blueberries (intense brain food with anthocyanins and antioxidants for recovery) topped with grated aged cheddar (intense brain food with dopamine precursors and saturated fats for those nerves) during and after pills. My pills go down better, and bit by bit the fog seems to be clearing.
Now that I might be able to think my way past a soggy Kleenex, it’s time to get that “activity” thing going again… if I can remember how. There is absolutely no substitute for activity, because it balances the autonomic system, improves neurochemical stores and their behavior, and can even reduce pain, with *no negative side effects* — as long as you don’t get hurt or over-do.
I had a dream last night of dealing with broken gym equipment, and of absolutely longing for good t’ai chi instruction. Until I find it, I’ll work with what I’ve got: my class notes and a couple DVDs from my old Academy. It’ll get me started, and then we shall see.
A friend I’ll call A died of suicide last night. It’s easy to say of people that they are rare and radiant souls once they’re gone, but A is the sort of person who was generally agreed to be a rare and radiant soul even when she was alive. Pretty angelic, really.
Suicide is a tough gig for all concerned, but being suicidal is living hell. I’m going to try to present some information in an accessible way, but this is an emotional time (it’s also deathiversary season for some of the biggest losses in my life, and there have been more deaths than usual this winter) … I’m very upset and very angry. It’s liable to show. Anyway, here goes…
Most of the time (not all the time), the deed that causes self-death is impulsive, which is the point of the 3-day hold in psychiatric hospitals: get them over that bump, then their coping skills come back, and then they find a way forward.
In cases like A’s, some survivors want to know why our loved one didn’t reach out, didn’t let us know ahead of time. Some want to know why this person “didn’t love us enough to stay.”
That’s a common feeling after suicide. These are all very common responses. Thing is, they miss the causative point.
Reality check
Here’s the thing:
Stop being so selfish!
It’s NOT ABOUT YOU. This is a tough one to swallow because you’re the one left alive and hurting, but it’s something to be faced in order to understand how this could happen.
It’s about being in so much pain that continuing is intolerable and there is no way this person can find to make it stop. Can you even imagine that? If not, then who are you to judge? If you can, then why are you blaming the victim?
Do you think she didn’t try hard enough, or know enough to battle this more effectively?
Actually, that’s a fair question. Some people don’t know enough, and need the chance to breathe, reboot, and find another way forward. (Most people who attempt suicide fall into this category.) It’s not an unreasonable thing to ask, so let’s look into that.
Some things can’t be fixed
My lovely friend A was a sophisticated, educated, well-informed consumer of, and professional in, the health care industry and effective alternative therapies. She really knew her way around.
I have a pain disease that, if I have to be truthful, hurts more every year. I’ve had over 15 years to ramp up to my present level of unthinkable, brain-blistering agony — and to find ways to manage it along the way. I can kid my mind most of the time that the pain is hardly there. I’m not likely to kill myself any time this year, though I might get flattened by a bus in a fit of absent-mindedness due to masking too much pain… you never know. (I’ll keep wearing bright colors and getting assistance around town, so don’t worry unduly, Mom!)
My friend A had a painful condition evolve recently that wouldn’t budge despite much work, and a surgery with… interesting characteristics. I sure don’t need to spell that out for those of you who’ve had, cared for, or performed surgeries. One of her main nerve branches was involved, which tells you the rest. It was risky, tough, and fraught. She knew that. Surgery was the only way to avoid the dreadful situation she faced if she didn’t have it.
By the time she made her last tragic decision, A could easily have been in a level of pain comparable to what I live with, but she did not have 15 years to ramp up. Most of that mountain of agony landed on her inside of a few weeks.
She knew what was going on in her body and worked for years to correct it without surgery.
She knew what the surgery might result in and she tried it anyway.
She knew her options.
She knew what to do to mitigate risk and optimize healing.
It’s likely that she did everything that could possibly be done.
It’s likely that there was too much pain and no way to escape it.
Sometimes, some things can’t be fixed.
I respect her choice. I hate it, it makes me miserable, but given the circumstances, I respect her choice as I respect her right to make it.
I don’t blame A. I wish that things had been different for her.
Please remember the compassion that was at the core of her spiritual and professional life, and return it to her as well as you can. She may need your compassion more than ever, because the end of her life was so awful, and she worked and fought so hard to make it.
She loved you. She loved us all, in her endless outpouring of loving-kindness and intelligence and determination. Please, try to give some of that back to her, now when it’s no longer easy.
Step Up
Of course you’re angry to lose wonderful people to suicide. Want to do something about that?
Vote for universal health care, so people like A can get timely care and prevent minor issues from becoming major ones and then becoming deadly nightmares. Because this should not have happened in the first place.
Lobby for universal housing and emergency accommodations in every state, so people like my brilliant friend Cross don’t have to choose between being murdered by a caregiver or taking their own lives, because NO OTHER OPTIONS EXIST.
Get your elected representatives to re-fund, and stop de-funding, mental health services and social safety nets, so my gifted friend Ethan didn’t have to shoot himself in the head to make the PTSD nightmares stop. Every dollar spent on these programs saves between 10 and 800 dollars in the costs of cleaning up the failures resulting from their absence. Our economy cannot afford that kind of constant, suppurating loss.
YOUR VOTING RECORD AFFECTS THE SURVIVAL OF THOSE YOU LOVE.
Don’t step into the voting box in the hope of choosing your next drinking buddy; the POTUS will never drop in at your neighborhood dive. Try to remember you’re voting for your next Chief Executive. This needs to be someone who’s smart enough and wise enough to do the job of leading a huge country that’s in serious trouble.
If you feel that, against reason and compassion, against economics and decency, you really have to vote against these policies or vote in those who oppose them, then don’t EVER complain to me about losing people you love to suicide, or maltreated illness, or poverty, or homelessness. These deaths are optional 99.9% of the time, and I have absolutely had enough of them!
This worm has turned
I used to be vigorously opposed to suicide. I spent too many hours coding people who had no choice about whether they lived or died, so that the occasional attempted suicides I treated in the ER just made the bile rise in my throat. Those idiots were bloody well going to live whether they liked it or not, and if they reached consciousness, they were getting a short and fiery talking-to from a short and fiery RN.
One day, I confided my thoughts to a longtime trauma counselor. She stopped me dead when she said, with great pain and exquisite kindness, “They do that because they can’t think of any other way to stop the pain.”
I tried to imagine so much pain and so much trapped-ness… and I couldn’t hate them any more.
And then, years later, I developed CRPS… then fibromyalgia… then dysautonomia… and, this week, I’m getting screened for a couple of cancers.
Those of you who follow this blog know that I spent a few years clinging to life by a thread. The pain, disability, and relentless, pounding losses and brutality of the world on the suddenly-disabled, on top of an ongoing roster of bereavements around me, very nearly finished me.
I was suicidal for some of that, only I was not going to screw it up; if I did it, I was going to do it properly. So there were no attempts, there was a thorough exploration of the idea. (At the very bottom of my personal root under the final level of Hell, I found … curiosity. I could not rest until I found out how this story went. Not only would I miss my funeral by several days, I’d never find out if we got a cure in my natural lifetime, if I ever figured out how to blog, what exactly CRPS is, who I had yet to meet, or anything. That was more unbearable than pain for me: unsatisfied narrative curiosity. I can’t explain it, I can only report it. I’m still working out how to crash my funeral.)
The point is, I’m pretty familiar with the landscape of endless pain.
I understand, with diamond-sharp clarity, that there is a point where a person simply shouldn’t have to put up with any more.
I know, as I never did in the innocence of my ER days, that there is such a thing as No More Options.
The word “unbearable” is no longer just an adjective; it has real meaning. Some things should not be borne, and that’s bad enough, but some things really cannot be borne. What then? Do we turn our backs and shrug, feeling we’ve done our jobs?
Those who’ve survived the suicide of someone you loved, you have my absolutely heartfelt sympathy. It’s awful, peculiarly and specially awful. There’s nothing like it.
If you’re really outraged, turn your anger onto a suitable target: the systemic failure that made that cherished person’s life unlivable.
That would honor them, in a remarkably constructive way.
I’m off to make sure I’m registered to vote tomorrow. I don’t want to sit this one out. I’m torn up and miserable, and I want to honor the memory of A and all my dear departed angels.
My desk setup is nonexistent and much of it still buried in unpacking. I wish I’d been writing some of the wonderful blog ideas that have passed through, but I didn’t. Rather than trying to reconstruct them from addled hindsight, I’ll just go on as if I had a whole nest of posts to plop this one into, and go on from here.
As my desk situation indicates, I still feel perched, rather than settled. I’m going to have to find a rental in the spring and then start looking for a miraculously good deal on a house to buy after that, so it’s hard to unpack all the way.
Moreover, California is still extending opportunistic tendrils into our wallets, task lists, and attention.
And then there are the periodic health crises: a bit of allergy exposure here, a bit of partner’s chest pain there, a sprained wrist from me overdoing, a sprained back from him overdoing… you know. Stuff.
Oh, and the holidays, with a trip and gifties to prepare, mostly for people I haven’t seen for over a decade… no pressure.
These aren’t excuses, they’re reasons. I don’t really believe in excuses; it’s largely an irrelevant concept. It’s for an injured party to decide if I’m excused, not me, so “offering an excuse” just doesn’t make sense. I have reasons, but so does everyone.
Here’s the thing I feel a need to mention my reasons for:
I’ve let my self-disciplines go. T’ai chi, qigong, meditation, reiki, relaxation exercises, stretching, even listening to chamber music — I think about them, but I don’t do them. I still have my morning routine, or at least half of it… if that… OK, yeah, my self-disciplines are pretty much out the window.
Like medication, meditation only works if you use it.
After weeks, actually months, of coping and managing with (and concealing, because that’s what chronically ill people do) my rising instability and neural chaos, I’ve finally started skidding off the cliff.
As for the effect… I’m trying to come up with a good image.
Imagine a patch of sea. I’m in a well-rigged little sailboat, noodling along in a fair wind.
The oil of willpower is constantly sprinkled on the water’s surface, keeping it smooth and flat, easy to sail along on.
Underneath, the weedy patches pluck at the propeller and keel, the barnacles grow restive and start plucking back, the creatures swimming underneath get bigger and more voracious, and then they get big enough to break the surface now and then.
More oil! Keep sailing!
Those surface-breaking tiddlers get chased off by the real mondo beasts. The boat is getting sprayed by the monsters breeching.
Everything’s fine, I’m too busy to pay attention, la la la la la I’m not listening!
Also, the wind is acting up. The boom is starting to swing across at head-height.
Just a little farther now! More oil! /BOOM/ It’s OK, I’m fine, just a flesh wound!
Unbeknownst to me (since I’ve got the radio turned off, because I’m not listening), there was a string of earthquakes.
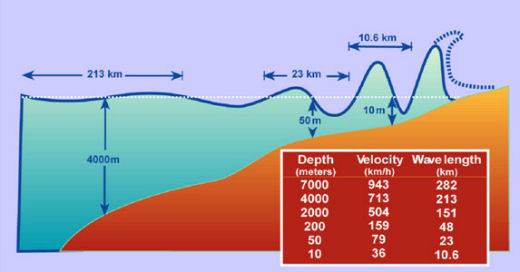
Since Banda Aceh and the meltdown at Fukijima, we’ve all learned about how earhquakes make waves. The shock of the quake trundles happily along the ocean floor until the ocean floor rises towards the shore. Then it sucks the landward water into itself and brings it all back as a tsunami.
If you’re afloat and listening, you move out to deep water, sail over the bump without losing stability, and you’re fine. If not… cue exciting sound track and hire George Clooney for the (possibly race- and gender-inappropriate) lead in another disaster movie.
There was a wave and I wasn’t in deep water. I didn’t handle it well; I was dysregulated and chaotic for days. Days. I was so dysregulated and chaotic I didn’t even see that that’s what I was, until it was pointed out to me — by the person who’d just gotten butt-kicked by an earthquake. That is not a fair burden to put on someone who’s already having trouble.
I have a personal meme about being good to friends. This is important for us spoonies (as chronically ill people sometimes call themselves.) My disease treats me like crap, but that isn’t a license for me to treat others like crap.
People who are protected from the true impact of this illness need to not get it at close range, or they run away (understandably) feeling as if they just got burned.
People who have this illness can understand a lot more, but are able to do much less.
I have to communicate appropriately. That’s my job in each relationship.
Basically, humans are emotionally fragile creatures and — whether I want to be judgmental about it or not — I can either respect that, keep the worst of my crap to myself, and have good relationships; or I can expect them to be as tough as me and to do so on my schedule, neglecting that they have to be as tough as themselves on their own schedule, and wind up isolated. Because I’m human too, I’m emotionally fragile enough that being isolated sucks.
I absolutely dropped my backlog of frustration and pain and rage on someone who was about the last to ever deserve it. That’s quite a breach of trust.
I stopped taking care of myself. As a result, I fkdup and hurt someone else. Now I have to own up (did that), figure it out (working on it), and do what needs to be done (re-integrate my practices) to prevent it ever happening again (and find a way to cue myself before I get bad: the missing piece.)
At that point, I’m allowed to make amends. It’s another tweak of my logic that I can’t make amends until I’m sure I won’t make the same mistake.
Being a spoonie is hard work. Part of that work is these time-intensive disciplines that seem like “oh how nice, you’re so cool, I wish I could do that” — but, as it turns out, are really not optional if I want to function.
Why I need to do my disciplines: to stay out of this pit with Allie.
BTW, do you notice how people excuse themselves by saying, “I wish I could do that”? I listen for these words coming out of my own mouth. It’s a sure flag that I’m throwing the baby out with the bathwater. Oh, a little extra effort up front to save a whole lot of trouble later on? H’mmm…
We all screw up at times. The consequences for spoonies can be life-threatening, if the wrong relationship gets ruined. Handling these issues is part of “living anyway” in the face of profound disease. It’s harder to figure out and harder to repair the damage, because of the nature of central nervous system diseases. So, dear reader, I’ll try to stay on the right side of the line between washing dirty laundry and discussing a common issue here.
We often tell each other, “You can’t take care of others if you don’t take care of yourself.” That’s a tough one for caregiver personalities; we’d much rather take care of others than ourselves. However, it was through failing to take care of myself that I actively hurt another. That is a whole different octave of problem. I guess I’d better learn this lesson.
This is a lot of thinking for a breached boat. I can do it, though. I must. I’m still a long way from harbor.
It’s not easy to find providers who can pay attention to the people in front of them and think their way out of a wet paper bag at the best of times, especially in the increasingly money-oriented and depersonalized model of care that grows and spreads out from the US like a bad rash.
When you’re looking for a specialist in a rare disease like CRPS, it’s even more interesting.
Sources for lists of providers
The online info-and-education site, RSDS.org, can send you a list of providers if you write to them and ask: http://rsds.org/finding-a-crps-specialist/. More usefully, though, they also provide a list of links to medical-specialist licensing board sites, where you can find specialists in your region.
I checked these out.
American Board of Pain Medicine
Enter your city, state/province, and country in the fields provided; choose your target category (Anaesthesiology, Physical Medicine & Rehab, Neurology, Psychiatry, etc.) to find someone board-certified in that specialty; and click Find. http://imis.abpm.org/abpmimis/abpm/directory.aspx
This very useful search tool includes a range of natural, ancillary, and supportive fields of care, not just physicians. It also allows you to set a distance, so you can expand or limit your commute as you see fit. https://members.aapainmanage.org/aapmssa/censsacustlkup.query_page
Last but not least
Of course, if your insurance provider has a specific list of providers they’re willing to pay for, you may have to start with the list they give you. That simplifies the process initially.
Using online reviews rationally
Having found a list of specialists, I strongly recommend reading lots of reviews to find the one who suits you the best.
That will be different for different people, of course, because we have different bodies and we each have found that certain kinds of things work best for us; doctors, likewise, have different brains and are inclined to use a distinctive set of treatments, believing that that is what’s best.
So, if possible, we probably want to find a doctor whose approach and treatments bear some resemblance to our own.
Excellence
In addition to that, I recommend finding someone with over a decade of practice. There is no substitute for experience. It’s the only way that judgment — that subtle sense that takes in a lot of info subconsciously to arrive faster at a better result — can develop.
Excellence takes time. Extensive research on excellence indicates that 10 years is the functional minimum to develop it.
Personally, I tend to go for 25-30 years. I know that I require a collegial relationship with my doctor, and it takes an unusual degree of poise for most specialists to handle that gracefully. Also, I really need to be treated by someone who knows more than I do, and the longer I have this, the rarer that is….
Once I get a list of specialists, it’s pretty easy to screen out the majority on the first pass, on the basis of inexperience or irrelevant experience. Some of these review sites, like ratemds.com and healthgrades.com, show the education, experience, rewards, and publication highlights for each physician. (All of this is public info.) These data make a great screening tool.
I only need to do in-depth review reading for less than a dozen doctors, usually. I don’t feel comfortable with less than 4 review sites for each doc I take seriously. Each site has its own slant, so I prefer to triangulate on each provider’s patient relationships from different sites.
Caveat emptor: It’s important to look at review sites with my brain plugged in and working. We know that some reviews are posted malevolently, and that everyone — including doctors — has a bad day. We also know that everyone — including doctors — has got their blind spots. That’s fine. I’m looking for PATTERNS, not exceptional instances.
For instance, one memorable doc treated beautiful people very well, and everyone else very dismissively. When his attention was engaged (which, for him, was about looks), he was intelligent, appropriate, and did outstanding work; these are valuable traits. Therefore, I’d recommend him (with an explanation), to friends who meet the age/BMI criteria in his sweet spot, because good care is good care — but I’d emphatically warn against him to the rest!
Last time, I wound up choosing a doctor who had a super high proportion of “he listens to me” remarks, had over 30 years of practice, had started in psychiatry (which indicated a more human-oriented and less problem-oriented approach, I thought), and did charity work for pain in his own time. That turned out extremely well. I wish I could get him to move across the country now, because I hate having to start the search all over again.
Now that I’ve got all my links in one place, it’ll be a lot easier.
Recap of my process
1. Create a list of potential providers:
Choose an appropriate specialty, such as..
anaesthesiology (training is oriented towards meds and procedures)
physical medicine and rehab (training is oriented toward physiotherapy and mental discipline)
psychiatry (training is oriented toward neurochemistry and life habits)
Choose an appropriate level of experience,with 10 years as my recommended minimum.
Make a comprehensive list of possibilities in your commute distance, using one of the board-certification bodies above or the list your insurance company provides you with.
2. Narrow it down to what makes sense:
First, quick pass through the list: screen for appropriate specialty (you’d be amazed at what winds up in those lists) and experience.
Second pass through the list: Start looking at online reviews. Cross out those who do a great job of pissing off their patients. Again, you’d be amazed… Every single doc gets a certain number of “he treated me like crap! I’ve never been so insulted in my life!” remarks, so I don’t notice a few of those, but when they predominate, out that doctor goes.
Third pass through the list: I look at 3-4 sites containing online reviews for the surprisingly short list of names I’ve got left. Some reviews are cut-and-pasted across sites, so I count those only once. This is where a pattern of personalities and approaches comes across.
Final triangulation: These impressions are easy enough to check by looking at the doctor’s web presence — activities they’re involved in, published work, what they do in their spare time (I find doing disease-related charities more compelling than golf club or Rotarian memberships, for instance), and I’m quickly down to 1 or 2 practitioners.
From there it’s a very simple choice.
3. Pick one.
If it’s a hard choice, I’ll call the office and ask to talk to the nurse. The staff a doctor hires have an awful lot to do with my experience there, so, by the time I know the doc has met my other criteria, incompetent or stupid staff is a perfectly reasonable deal-breaker.
I’m willing and able to travel quite a distance for a good provider, and this makes it a lot easier for me to find one. I’m deeply indebted to my partner for being so willing and happy to do so much driving on my behalf. It makes an enormous difference, and I’m suitably grateful.
I hope you all can find the right doctor where you need one. There is simply no substitute for good and appropriate care.











.png)
