New series: Quickies. Short, practical notes, mostly about things to try for problems with CRPS, dysautonomia, mast cell & histamine disorders, etc.
Problem
I get what my grandmother would have called chilblains: cracks in the calluses around my feet and sometimes on my fingers. Nasty, uncomfortable, and — because they’re surrounded with thick walls — hard to heal.
Option
I’m an old nurse. I know a lot about healing wounds of all kinds. Nothing worked, at all …until I tried Ching Wan Hung, in the copper-colored packaging.
Ching Wan Hung: Different manufacturers but similar copper packaging
It’s a traditional herbal product with Chinese cinnamon, which smells a whole lot different from the tropical stuff we eat. It also has menthol, which I can’t tolerate normally, but is no problem for me here. I can scarcely smell it, so maybe it’s a dosing or production issue. Most herbal salves bring on menthol like a battering ram.
Usage
I squish it right into the cracks and holes of the sores, rub it in well, then put a dark sock over it for an hour. (It stains light colors.) Then I get on with my nap, or my task, or whatever. I put it on twice a day, before getting out of bed and at bedtime. I should probably use it more often for faster results, but I’m not very good at that.
It doesn’t work for everyone, just as everything else I tried, that did work for other CRPSers, didn’t work for me. It’s another option.
Sourcing
I’ve found it online at the usual places and at my local Asian/ international market, usually in little copper-colored tubes, which is more hygeinic than the larger tub you have to stick fingers into. It’s cheap for what it is, too.
You can ask for “Chinese burn cream” if you can’t remember the name.
Caveats
Use common sense (all my readers are extremely sensible, so of course you will).
If it brings up a rash or makes you wheeze, wash it off well and never use it again. Not for wounds that bleed readily or might be infected. Never use on bites, because mouths are utterly filthy and bite wounds need different care. If you can’t feel the tissues where your chilblains or non-healing sores are, see a doctor about them and follow their advice over mine. And so on.
Spoonies, you know how we sometimes drift through the day? If we don’t have an external demand shaping our efforts — kids, work, methodical spouse or housemate — then, for some of us, getting through the day can be a matter of bumping or lurching from one need to the next (use toilet, refill water, rustle up food, manage an appointment, negotiate for a ride, do the self-care things that require that up-front energy to make them happen, organize recovery periods from each of those activities…)
Yeah.
An old friend of mine reminded me that there can be a thread running through the day, in addition to the usual “what’s the next task for survival and coping?” —which, let’s face it, gets a bit grim.
We can suggest to ourselves what that day’s thread might be.
This can line our attention up on it, and make the day less annoying and, in some ways, more fruitful. It also comforts the brain & spine with a sense of supportive purpose.
That’s worth a lot.
I mull it over the night before and find myself with a short list. Next morning, I pick one or two.
This also gives my brain/mind the supportive sense of being cared for at the beginning and end of each day.
I picked two this morning, but I can only remember one: calm. Picking “calm” as the thread for today is particularly good, because there’s a lot to do before I get a molar cut & chiseled out of my head with hopelessly inadequate pain control this afternoon, and thinking about that is not calming, but it’s going to happen and it needs to happen. I get to figure out how to mitigate the horror and so forth, and stay in my skin (so to speak) while I prepare for a testing few days of hard recovery.
Because I chose “calm” for today, I’m taking the time to write this, instead of trying to cook soft food, drag out the vacuum, shower, and make tea & take my pills, all at the same time. And doing all of them badly, if at all.
This word for today is providing a good anchor to hang onto as anxiety and the foreshadowing of so much more pain tries to wreck my mind.
It’s not that things are going to be anything other than what they are. It’s just that it’s not actually the end of the world, the wound will heal, and I can weather that process. I remember that when I reach for the word and idea of “calm”.
This is the 4th day and the 4th word since that conversation. It has improved my ability to get things done that are time sensitive, and it’s helping a lot with getting through this testing day.
I used to do this years ago. It’s amazing what we forget.
I’ve already vacuumed and breakfasted, and did them well enough (my vacuuming kit is in the picture below. Check out the padded suede gloves to cut the vibration from the handle!)
Now for tea, pills, quick washup. This is do-able.
This is about the messy intersection of CRPS & the mechanical aspects of central nervous system dysfunction, and dealing with those effects.
I’m writing through the waunnng, waunnng, waunnng of a ringing headache. I’m hoping that if I hydrate, urinate, and (carefully) ambulate enough, it’ll pass faster. We shall see. Meantime, I’ll do my best to pass on some useful info.
The brain and spine are supposed to float in cerebrospinal fluid. We are supposed to stay hydrated enough to keep those sensitive tissues from grounding out.
We have 2 kidneys – each one capable of filtering twice the water we actually need – as a practical accommodation for the fact that, throughout history, most water was filthy and needed lots of filtering.
We have 4 times the kidney power we need for a busy, messy lifetime. We’re supposed to use them! The more we use them, the healthier they can stay. They love to do their job.
When we’re properly hydrated, our brains and spines can float comfortably in their spaces. When they float comfortably, they have plenty of shock absorption protecting them.
Spinal care
Dr Faye Weinstein taught me an important part of brain & spine care.
I had too little cartilage in my knees, so I had developed the habit of dropping into chairs instead of using my legs to lower myself neatly.
She hated that. She visibly flinched, and one day she finally cried out in audible distress, “Stop doing that!”
I stopped doing that.
Just as she had predicted, my baseline level of misery became less.
Once I was out of the habit of dropping into chairs, then, when I did it again, it caused headaches and sometimes back pain (depending on my hydration, of course). I was no longer used to enduring this as part of my daily quorum of yuk.
That was (checks watch) over 10 years ago. My brain and spine, oddly enough, haven’t gotten any younger since then.
Yesterday (after a couple of days of being “too busy” to hydrate properly), while I was turning to admire something across the street (a boat or a building; I forget which)… I stepped off a step I hadn’t noticed. One step down, caught myself, barely stumbled, no harm done. Massaged my neck a bit, to ease the slight jamming on one side. In my formerly healthy system, that would have been that. Probably would have forgotten about it instantly.
But now is different.
It took 10 minutes for the icky feeling to set in at my low back and back of head. It took a little over 2 hours for the whole brain-fog and uncontrolled body pain to take hold. Chronic CRPS really is wired into the whole neurological system, and one of the hallmarks is how the spine takes on an anti-life of its own in the face of any signs of disrespect.
Clearly, my spine felt seriously disrespected.
Content warning – skip this description if you’re squeamish about pain:
We know that I have no effective pain control left to me, with genetic tweaks making narcotics disgusting (they make the pain worse, cause untreatable nausea, and trigger horrific mood swings), and mast-cell activation making NSAIDS unbearable (they cause a soft-tissue-wide inflammatory pain, making it feel like shards of hot glass are hammered into all my cells).
So, how to approach this?
There’s a super-concentrated lemon balm extract that helps calm down inflamed nerves. Lemon balm has been used to calm nerve inflammation & pain for, approximate thousands of years.
Since all the nerves coming out of my spine are feeling very hot right now, I’m taking that about every 8 hours.
Note: check this against your meds, especially with GABAnergics. Ask your pharmacist to check their standard herb-drug interaction charts.
Pain salve on my spine and up my neck before bed, and also on arms/ shoulders and hips once I tried to sleep, helped noticeably.
It was a rocky night, but I’ve been getting as much water down as my tummy will tolerate and, now that my kidneys have been flushed 3 times, the headache is noticeably easing.
Conclusion
We can’t be alert every second. Our senses are so distracting at the best of times. Finding ways to manage these impacts is unspeakably important.
Long-term pain patients tend to get self-concerned to a degree that could be obnoxious normally, but it’s a legitimate self-care attribute in a life where one wrong move or one wrong exposure can destroy weeks or months of work.
Image by neurollero on flickr, CC share-alike attribution license.
One benefit of this self-attention is learning how to manage and mitigate the problems that arise by catching them early, and sharing the info in the hope that it’ll do some other painee or their caretakers some good. We have to learn from each other. Nobody else is as qualified.
I headed to psychotherapy after texting, “I’m on my way. I’ll see you in person today, barring the unexpected”
I was feeling a bit cautious, because a couple hours before, the thought had come to me, “when things get hectic, trust your training.”
What training? Was I about to have a series of intrusive thoughts harking back to the times I’ve had to file restraining orders, one of which magically disappeared and I had to flee the area – right before Christmas? I hoped not. Martial arts training has certainly come in handy, but come on…
No, no intrusive thoughts, but I did wonder which set of training I should have in mind.
A few miles down the interstate, I saw a pickup truck stopped dead, and a sedan facing it.
People were only just getting out of the truck. I put my flashers on and pulled in behind.
I definitely trust my training in this kind of situation. I put my anxiety to one side and sailed in.
The only person to worry about was a littlie in the back of the sedan. Had spontaneous pulse – a good one – and respirations. He could speak, to the limit of saying, “I want my Mommy” (sound of heart-strings tearing), so I checked his spine at his neck. It was there, but not quite right. Once he could speak more, he told me his neck hurt where I touched it (I’d been holding his head & neck stable since I felt it). As I told the fire department medic later, “on me, it’d be a chiropractic adjustment. On a littlie that age, I’m not sure.” He nodded and sent his buddy in with a pediatric cervical collar.
Littlie’s mother was on the phone the whole time with him. So much love swirling around in that car. I told the Dad that I noticed it, and that it’s healing.
At each stage – or rather, just before the next round of excitement – I explained to Littlie that there would be more people, highly trained people who really cared about him being okay. Let him know roughly what to expect at each stage. Coached him to go along with things as well as he could. When the fireman asked him to squeeze his finger, he squeezed my hand instead (sound of heart melting).
I could see most of my words going over his head (as expected), but I could also see the sense of reason and structure calming his exhausted and shocky brain so he could tune in a little more.
I grew up in a musical household, so naturally I hummed pretty little made-up tunes and it visibly calmed him – and possibly his parents too, a little.
I’ve been working on learning how to stabilize a shocky system for 25 years, on top of my trauma nursing work. I’m only a patient – and a nerd – but still, I have lots of good training. I trusted my training in that, too.
I gave his mother my number right before the fire department and EMTs rolled up. I think it was a training day, because there were 7 or 8 more people there, one of them a cheerful charming know-it-all (every team needs one of those) who got the best responses out of Littlie.
I let the kid know I had to go but his Mommy would stay on the phone with him and he’d be cared for by these really nice people. Told his Mom I loved her kid and he was terrific (sound of heart-strings pulling).
Once his c-collar was on (definitely a training day; I helped get it positioned and sealed correctly in the end) and they had the gurney ready, I realized I had to stand up. After perching my crippled butt by one hip on a steel door frame for half an hour. In front of people. Specifically, a total of 9 or 10 fit, athletic slabs of beef (-cake) no less than 10 years younger than me, and most of them half my age.
This was not going to be great for the ego, but I knew I could get a laugh out of it.
So I used both arms and every available leg (which was slightly less than 2) to lever myself upward, saying, “I’m an *oooold* trauma nurse” by way of cover, and squirmed through the kindly, protective testosteronic press and into fresh air.
I signed off with everybody and retreated to my comfy car.
I called my psychotherapist and said, “Remember what I said about ‘barring the unexpected?’…”
We had a phone session once I was safely off on a side street and in a proper parking space. She was full of commentary about how I applied those psych skills and met psychosocial and informational needs appropriately, as well as the nursey stuff. So yeah, that was good…
… because my brain was churning constantly about every single moment and thought and decision for an entire hour. Looking for a fault. Looking for something I’d missed or where my training had lapsed or been forgotten. Cycling through, over and over, looking for any lapse.
This used to be how I improved my skills – look for errors, even tiny ones, and figure out how to prevent or avoid them in future. Now, it’s just my ADHD brain torturing me.
And computer says Nope. Failed to suck. I’m pretty sure I failed to suck. That’s a relief.
I’ve been thinking about it pretty much nonstop, but rather than worrying myself woolly, I got an organizing thing for my car and picked up some food. Both of these are calming, grounding things, perfect for pulling my adrenaline out of the stratosphere.
Then I crawled home and had fresh corn and gluten-free carrot cake for dinner. It’s good to have a little sweetness when your body is still convinced the world is full of excoriation.
I’ve had no calls from them and I don’t expect one. They’ve got to be absolutely wrung out regardless of how things went. The kid comes first, and then comes their own care and self-management.
They don’t have to think of me ever again: I know how shocking and painful it could be to revisit the moment.
I’d love to know. I hope like crazy that the kid came out of it OK. I never got to follow up with patients when I was a nurse (because confidentiality), and I’d sure appreciate it if this family wanted to give me a heads-up just to soothe that old itch.
All that being said, I want all you non-nurses to know that they don’t owe me one word of contact or one moment of concern. I was in the right place at the right time with the right training, and I trusted my training. That’s what we do.
They have the hard part: figuring out next steps with a shook-up and possibly injured Littlie who was going home early because he was already ill.
That kid was having a rotten day.
I sure hope it got better.
Forestalling future problems
I don’t have a jump-kit for my car. That could be a problem in the future. I was lucky this time because all I needed was my brain, arms, hands, and voice.
It’s probably the 6th or 7th accident I’ve stopped at and I really do know what’s needed at the roadside – and it isn’t much. I used to get confused by the fact that I didn’t have a stethoscope, oxygen on tap, i.v. gear, and All Tha Meds. Once I’m on scene, though, it gets very easy.
Any blood or, indeed, anything wet? Nitrile gloves, packed up in pairs and stowed in a closed outer pocket to keep them clean & dry and easy to get on.
Heaven forbid, does anybody need CPR? This very rarely happens, but when it does, I don’t want to have to dig for the needful. I physically can’t do chest compressions (though I can coach any able-bodied person properly) but I can darned well use a mask with a one-way valve as if I’ve had years of practice. Years. You don’t have to have that (the training has shifted away from doing rescue breathing) but I feel that I do.
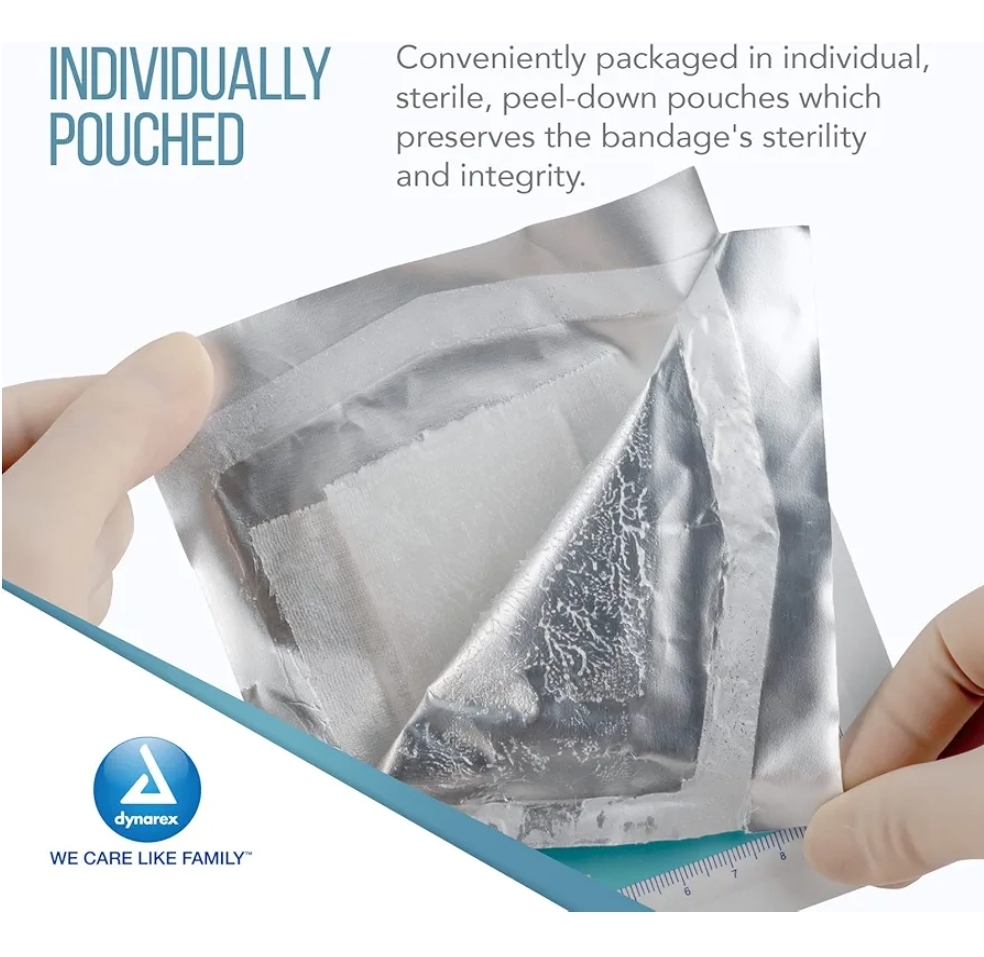
Pressure dressing? Kerlix. Sling? Kerlix. Wound cleaning? Kerlix makes a great sponge. Wound wrap? Kerlix. Piece of clean water-resistant paper to slap over a bubbling wound? Wrapping off a Kerlix.
So, plenty of Kerlix.
Road rash? Plenty of saline rinse (and a Kerlix) then a petroleum dressing to stabilize the damage until the ER can do a better job.
And possibly most essential: disinfectant cleansing towels, individually wrapped and big enough to grab. Those get used before if there’s time, during if the patient wants cleaning up, and definitely afterwards.
Because allergies & neurological reactivity, I stick with ethyl alcohol 70%.
Secure the mess. A gallon-sized zip bag or 2 for garbage and wrappings. Having a garbage bag is one of the things that separates rescuers from ego-trippers.
Oh, did I say that out loud? Sorry. I don’t want anyone not to stop & help… I just wish that, if they’re going to the effort of bringing gear, they could pick up a bit. Seeing blood and mess is not good for survivors & passers-by.
I got all these online for about $10 each, and also got a clear bag (with outside pockets) to put the kit in.
I’ll keep backstock at home.
What I don’t carry
Blood pressure readings, stethoscopes, and pulse oximetry are at-home and in-hospital concerns: we want to know if what we’re doing is working over time and refine our understanding of the body’sfunctional state.
In the field, the main issue is not whether the patient has rales or a murmur, but whether the lungs and heart are keeping them alive – a much simpler, larger-grained issue.
So, these tools might be nice to have, but for a noodle-noggin like me, they’re an added complication and a bunch of expensive equipment to lose at the scene.
In the field,
You need to keep pulse and respirations going,
the spine stable,
make sure the inside stuff stays inside
and in place,
and (as much as possible) the outside stuff stays out – or at least doesn’t move much where it’s inside the person.
And that, ladies and gentlebeings, is Advanced First Aid and Basic Life Support in a nutshell. You’re welcome 😊 Now go get that training… please?
On my 21st birthday, I went out with a bunch of women friends, including 2 couples. All of us health-care workers. Drunk jerk got thrown out of a car right behind is as we stood on the sidewalk deciding where to go next.
He decided that us being out without a man, and clearly happy in our own company, was a terrible transgression. Then he noticed the couple vibes. Then he called us “a bunch of” d-word. Then he tried to kill one of the women in a couple.
Someone else saw him draw a knife. He went to slash her throat. Someone else pulled her back, by her arms unfortunately.
I saw him raising a fist to a defenseless friend, her eyes huge, staring at the fist.
Somehow I levitated between 2 parked cars and a couple meters of pavement in the time it took his hand to move another foot.
I landed in front of him with my arms raised in a blocking stance my Dad taught me at 9 or 10 years old. He said, “I’m teaching you to block with both arms at once, so you don’t get confused in the heat.” That worked!
The attacker looked stunned. Took a step back. I stepped back. He took another, one more, then turned and ran.
I ran back to the bar we’d come out of, passing a couple of delightful young men, shouting a warning: “There’s a man, with a knife, back there.”
I had no idea my left side was covered in blood pouring out of my face.
Those two precious darlings ran. Found out later they ran *towards* the attack, followed my friends’ pointing fingers, and kept him blocked in at the train station, where he had just missed the last train out. Trust me, it takes balls to be a queen.
When the back door of the bar finally opened, the barkeep peeped out and said, “Sorry, we’re clo — oh, dear — somebody get me a towel with ice in it!” He clamped it to my face and that was the moment I realized my left shoe was squishing with the blood in it and I kinda lost my cool.
I hammered on the brick wall with my bare fists, screaming “Never again! Never again!”
I had already been a female for 21 years, which taught me a lot about uninvited violence; had learned about the Stonewall riots; knew the horrific statistics of how often non-heteronormative women are attacked “to teach them a lesson”; and had started getting involved in “let’s all treat each other like frkn human beings & not torture and kill each other like it’s a sport” types of activism.
So. All that was behind that “Never again”. It was too much in my life already, and I was barely an adult.
When the cops brought the attacker in the bulletproof squad car, so I could identify him, I couldn’t see at first because his hand was over his face. Cop went around to the side to ask him to lower his hand. He turned sideways, and I saw the profile that had gone to sink a knife into the throat of a defenseless woman.
It seemed logical at the time that I didn’t want to fight the cops, one on either side of the car. I decided to go through the windshield instead. It was only bulletproof glass; between fingernails and fury, I saw no reason (in my state at the time) not to get through it.
A minute later, with drunk dude stark white and frozen with terror, one of my friends (an ER nurse) pulled me off the hood by the slack of my best black jeans (this was the late 1980s) now smearing blood on the hood of the car.
She and the cop looked at each other and chorused, “I think that’s a positive ID.” ?
While this makes a great story, the memory of it also makes it very, very hard to speak up against microaggressive b.s. because you never know where it will lead. Name calling can go anywhere. Being in a group is some protection but not as much as you might think. If I’d tripped on my gods-assisted leap across that distance, my friend would be dead, and her partner would not have been even acknowledged as a widow, and all of us would have been stuck with that harrowing memory with no tolerable ending.
I now have long hair and am not nearly as fit, so I have the leverage of obvious straight privilege more than I ever did before. (Not that I’m personally wedded to gender or orientation. Binarism is a bit weird to me, but hey, you do you.) My actual sexuality has been all over the map and is currently parked in Neutral: don’t have it, don’t want it. But hey, you do you — that’s the bottom line.
That language changes all the time. When I was an activist, at first “queer” was an all-embracing term, but then the language started moving to an acronym. In the move to acknowledge all the variety, that acronym has gotten unwieldy. The English language being the adaptable thing that it is, another word-based term will emerge to act as the modern umbrella term; that’s still in process.
You don’t have to like LGBTQAI+. If you’d actually read, as I have, holy books in an intellectually responsible translation, you’d find that the major ones are OK with it. God is OK with it, but you do you: just keep your hands to yourself.
You don’t have to support LGBTQAI+ businesses or like having LGBTQAI+ employees. If you check the stats, you’ll find that businesses with strong LGBTQAI+-positive policies and culture get more and better work out of ALL of their employees. A tolerant environment is very freeing to everyone, not just the nominally unusual! But you do you; just keep your hostility to yourself. It’s not OK to be hateful or spiteful at work.
You don’t have to want a LGBTQAI+ family. If you check the records, you’ll find that kids raised in LGBTQAI+ homes are just as smart & just as competent (and generally somewhat more adaptable) as anyone else’s kids. You do you; just keep specific laws off those bodies, because it’s no more your business than your sex, your private parts, your children, and your home life belong in other voter’s hands.
You do you. Let others do them. That’s basic humanity.
It’s not just LGBTQAI+ people who suffer for it. It really is a disservice to everyone.
Let’s get this crapshow turned around, because we really need to get together on issues beyond the personal, if any of our descendants are going to have a bearable future.
Oh boy, another brain dump … This one on how to work on getting worsening tendinitis to back off and let you get your life back.
=================================== I’ve been through the worst possible scenario that started with this kind of overuse pain, and the worst possible things went wrong just short of amputation, and my entire life got wrecked.
Also, I was a nurse, and what with one thing and another, I think I’ve seen a lot of ways this can go. So, I do hope you’ll forgive me for offering some perspective and advice from the sharp end. It’s wholly well-intended and very much from the heart. I do not want anyone to go through a tenth of what I did.
Firstly, it’s usually possible to rehabilitate tendinitis, IF you are sufficiently wise and adult about it. (Easier said than done!)
Secondly, doing so takes time; give it 2 years, considering how widely it affects your life right now.
Keep in mind… *those two years will pass anyway.* Wouldn’t you rather be better at the end of them, rather than facing a lifetime of being handicapped in all the most fundamental and enjoyable tasks of life? Trying to live without using your hands is no way to go. Trust me on this.
It will require changes, some of them major adjustments, and some of them minor adjustments to what you already do.
There are several aspects to address, none of which are optional, but all of which have different things to try:
– Positioning during the day (when we do 95% of our activity.)
– Positioning during the night (when we do 80% of our healing!)
– Rest & recuperation time (without this, nothing improves for long.)
– Rest & recuperation physiology (nutrition & pain control.)
– Adapting life tasks to ease up on your wrists (this requires professional help to get started with, so the physical dynamics start off right and you learn what “good enough” really is and what it isn’t.)
You’re obviously a very bright and rational person, and I feel very shy about stepping forward here, but you’re doing what I did and what many people do, and smart and well-informed as you are, it’s just possible you’re overdoing to the point of damage, and that damage IS almost certainly recoverable and possibly totally preventable. It just takes a bit of time and work first, then you can get back to the best and most important things when you’re better. (Never give up on getting better.)
– Positioning during the day
Talk to your doc or physiotherapist about whether a brace would help or hurt your wrists. It depends on where the tendinitis is and what the triggers are. Alternatively, learning to tape them may be better. (I got a whole extra 6 months out of my right wrist with strategic taping.) The right structural support can change things. (As can the wrong structural support, but not in the good way.)
I assume you’ve been to your doc and have discussed that 🙂
– Positioning during the night
Few docs know this trick (my surgeon did), but it’s absolute gold: Wrap towels around your elbows at night so you can’t bend them up in your sleep. Since >80% of recovery and healing happens during night-time sleep, the more you can protect your arm tissues during that period of time, the better. Bending them up cuts off that process. Simply cuts it off. So, unbend.
Since you have this tendinitis, there’s a ~90% chance you sleep with your hands tucked up by your face. It will take some adjustment (sure did for me) but that position is about to change. You clearly depend on your wrists too much to let this go on, so *let* the nerve and tendon pathways heal at night, and see what that does for you over time.
This one thing alone has “cured” some people of their daytime symptoms. It’s terribly important — it repays perseverence.
– Rest & recuperation time
Yup… put the hooks, needles, etc., down for a few weeks to a few months. I’m sorry, but healing takes time and there’s no shortcut to this. The good news is, the time WILL pass, and you’ll be better for it. (I wish I’d done that!!!)
The most helpful guidance on “how long?” is probably from a rehab speciallist called an occupational therapist. They’re technically similar to physiotherapists, but they focus on the mechanics, tasks, and demands of daily life. THey’re more dialed into the practical application of the larger issues that physiotherapists and physicians work in.
Since you’re still doing these things despite the pain, I figure your doc may not be *completely* up to date on just how much this is interfering with your life and activities. I’m an old nurse; I’m not wild about doctors; however, this is a great time to get re-acquainted with yours — because he or she can sign you up for OT and PT to help you rebuild your tendons without further damage, and rework the hand-tasks of life so the *overall burden* of wrist-stress is better distributed and *still* gives you time to do the things you love to do!
– Rest & recuperation physiology
Tendinitis can be solely due to overuse, or it could be due to overuse plus other factors. (E.G., I have a fairly normal variation in my radial muscle, where the edge of the muscle bundle is sharp; it wound up scraping and irritating my radial nerve so much along that edge that I had to have a chunk of the muscle cut out. I also had carpal tunnel space that was simply tiny. That had to be opened up so the nerves and tendons could fit without hurting each other.)
Basically, if something mechanical really needs to be dealt with, it’s wise to deal with it so you can get on to the good part — getting better. (I’m no fan of surgery either, but sometimes it makes sense.)
Pain makes your body tissues sticky, and sticky tissues get gummed up; gummed up tissues hurt more because they can’t move right or work right or clean themselves up properly. And round and round we go.
Thus, less pain with better hydration (to clean out the sticky stuff, quite literally) makes for better healing. Two things can have significant effects on pain — nutrition and medication.
Wild fish and grassfed butter (bring on the Kerrygold!) are known to reduce inflammation, improve metabolism, and support healing. (Conventional butter and farmed fish, sadly, do not. Long explanation r/t histological metabolism.) Produce of all colors make a huge difference in healing.
Even with a great diet… in our modern messy world, and with a fairly longstanding pain issue evolving, it’s not ideal to depend on the finite number of calories you can eat to get all the nourishment your body is hoping for. Fish oil (very fresh: Nordic Naturals and Kiva are known to have good fresh processing and delivery methods) and, of all super-easy things, vitamin C are outstanding for inflammatory pain and nerve healing. As a long-time painiac, I recommend 500-1,500 gm daily of Ester-C, because it releases itself slowly and is the most digestion-friendly vitamin C I’ve ever used. Vitamin C works by refreshing all the other antioxidants. Wonderful stuff. Your nerves are among the biggest producers and biggest users of antioxidants; right now, they need more, but can produce less, so it helps a lot to make up the deficit.
From my own standpoint, I consider a good food-based multivitamin essential, because I’ve seen in myself and in so many others just how much of a difference it makes in healing time and recovery completeness. However, I realize many have strong feelings about supplementing with multis, and I don’t want to seem contentious 🙂
Ibuprofen/paracetamol, where you’ve got plenty of hydration and good nutrition, are terrific for reducing inflammation and knocking back the pain, of course.
– Adapting life tasks to ease up on your wrists
So you get to keep them for the rest of your life 🙂
This is where you want to start with an Occupational/Physical Therapist, rather than doing the natural/easy thing and trying what your friends have tried.
Why’s that? Easy — because of muffled signals. Since you’ve been dealing with this for awhile, you’ve gotten pretty good at ignoring some body signals, and one thing these pros can do is help you learn *which* signals are right, and which ones can be safely ignored. Once you get the parameters in mind, then you’re better equipped to choose your own adaptive gear from there.
Having the outside pair of eyes, which are so well-educated, is a great help in readjusting life and redistributing the load on your body.
I hope that’s helpful, and I hope you don’t mind my hopping onto this so enthusiastically. It’s my mission, now that I’m on borrowed time, not to let anyone else endure any of the horrors I did
A friend I’ll call A died of suicide last night. It’s easy to say of people that they are rare and radiant souls once they’re gone, but A is the sort of person who was generally agreed to be a rare and radiant soul even when she was alive. Pretty angelic, really.
Suicide is a tough gig for all concerned, but being suicidal is living hell. I’m going to try to present some information in an accessible way, but this is an emotional time (it’s also deathiversary season for some of the biggest losses in my life, and there have been more deaths than usual this winter) … I’m very upset and very angry. It’s liable to show. Anyway, here goes…
Most of the time (not all the time), the deed that causes self-death is impulsive, which is the point of the 3-day hold in psychiatric hospitals: get them over that bump, then their coping skills come back, and then they find a way forward.
In cases like A’s, some survivors want to know why our loved one didn’t reach out, didn’t let us know ahead of time. Some want to know why this person “didn’t love us enough to stay.”
That’s a common feeling after suicide. These are all very common responses. Thing is, they miss the causative point.
Reality check
Here’s the thing:
Stop being so selfish!
It’s NOT ABOUT YOU. This is a tough one to swallow because you’re the one left alive and hurting, but it’s something to be faced in order to understand how this could happen.
It’s about being in so much pain that continuing is intolerable and there is no way this person can find to make it stop. Can you even imagine that? If not, then who are you to judge? If you can, then why are you blaming the victim?
Do you think she didn’t try hard enough, or know enough to battle this more effectively?
Actually, that’s a fair question. Some people don’t know enough, and need the chance to breathe, reboot, and find another way forward. (Most people who attempt suicide fall into this category.) It’s not an unreasonable thing to ask, so let’s look into that.
Some things can’t be fixed
My lovely friend A was a sophisticated, educated, well-informed consumer of, and professional in, the health care industry and effective alternative therapies. She really knew her way around.
I have a pain disease that, if I have to be truthful, hurts more every year. I’ve had over 15 years to ramp up to my present level of unthinkable, brain-blistering agony — and to find ways to manage it along the way. I can kid my mind most of the time that the pain is hardly there. I’m not likely to kill myself any time this year, though I might get flattened by a bus in a fit of absent-mindedness due to masking too much pain… you never know. (I’ll keep wearing bright colors and getting assistance around town, so don’t worry unduly, Mom!)
My friend A had a painful condition evolve recently that wouldn’t budge despite much work, and a surgery with… interesting characteristics. I sure don’t need to spell that out for those of you who’ve had, cared for, or performed surgeries. One of her main nerve branches was involved, which tells you the rest. It was risky, tough, and fraught. She knew that. Surgery was the only way to avoid the dreadful situation she faced if she didn’t have it.
By the time she made her last tragic decision, A could easily have been in a level of pain comparable to what I live with, but she did not have 15 years to ramp up. Most of that mountain of agony landed on her inside of a few weeks.
She knew what was going on in her body and worked for years to correct it without surgery.
She knew what the surgery might result in and she tried it anyway.
She knew her options.
She knew what to do to mitigate risk and optimize healing.
It’s likely that she did everything that could possibly be done.
It’s likely that there was too much pain and no way to escape it.
Sometimes, some things can’t be fixed.
I respect her choice. I hate it, it makes me miserable, but given the circumstances, I respect her choice as I respect her right to make it.
I don’t blame A. I wish that things had been different for her.
Please remember the compassion that was at the core of her spiritual and professional life, and return it to her as well as you can. She may need your compassion more than ever, because the end of her life was so awful, and she worked and fought so hard to make it.
She loved you. She loved us all, in her endless outpouring of loving-kindness and intelligence and determination. Please, try to give some of that back to her, now when it’s no longer easy.
Step Up
Of course you’re angry to lose wonderful people to suicide. Want to do something about that?
Vote for universal health care, so people like A can get timely care and prevent minor issues from becoming major ones and then becoming deadly nightmares. Because this should not have happened in the first place.
Lobby for universal housing and emergency accommodations in every state, so people like my brilliant friend Cross don’t have to choose between being murdered by a caregiver or taking their own lives, because NO OTHER OPTIONS EXIST.
Get your elected representatives to re-fund, and stop de-funding, mental health services and social safety nets, so my gifted friend Ethan didn’t have to shoot himself in the head to make the PTSD nightmares stop. Every dollar spent on these programs saves between 10 and 800 dollars in the costs of cleaning up the failures resulting from their absence. Our economy cannot afford that kind of constant, suppurating loss.
YOUR VOTING RECORD AFFECTS THE SURVIVAL OF THOSE YOU LOVE.
Don’t step into the voting box in the hope of choosing your next drinking buddy; the POTUS will never drop in at your neighborhood dive. Try to remember you’re voting for your next Chief Executive. This needs to be someone who’s smart enough and wise enough to do the job of leading a huge country that’s in serious trouble.
If you feel that, against reason and compassion, against economics and decency, you really have to vote against these policies or vote in those who oppose them, then don’t EVER complain to me about losing people you love to suicide, or maltreated illness, or poverty, or homelessness. These deaths are optional 99.9% of the time, and I have absolutely had enough of them!
This worm has turned
I used to be vigorously opposed to suicide. I spent too many hours coding people who had no choice about whether they lived or died, so that the occasional attempted suicides I treated in the ER just made the bile rise in my throat. Those idiots were bloody well going to live whether they liked it or not, and if they reached consciousness, they were getting a short and fiery talking-to from a short and fiery RN.
One day, I confided my thoughts to a longtime trauma counselor. She stopped me dead when she said, with great pain and exquisite kindness, “They do that because they can’t think of any other way to stop the pain.”
I tried to imagine so much pain and so much trapped-ness… and I couldn’t hate them any more.
And then, years later, I developed CRPS… then fibromyalgia… then dysautonomia… and, this week, I’m getting screened for a couple of cancers.
Those of you who follow this blog know that I spent a few years clinging to life by a thread. The pain, disability, and relentless, pounding losses and brutality of the world on the suddenly-disabled, on top of an ongoing roster of bereavements around me, very nearly finished me.
I was suicidal for some of that, only I was not going to screw it up; if I did it, I was going to do it properly. So there were no attempts, there was a thorough exploration of the idea. (At the very bottom of my personal root under the final level of Hell, I found … curiosity. I could not rest until I found out how this story went. Not only would I miss my funeral by several days, I’d never find out if we got a cure in my natural lifetime, if I ever figured out how to blog, what exactly CRPS is, who I had yet to meet, or anything. That was more unbearable than pain for me: unsatisfied narrative curiosity. I can’t explain it, I can only report it. I’m still working out how to crash my funeral.)
The point is, I’m pretty familiar with the landscape of endless pain.
I understand, with diamond-sharp clarity, that there is a point where a person simply shouldn’t have to put up with any more.
I know, as I never did in the innocence of my ER days, that there is such a thing as No More Options.
The word “unbearable” is no longer just an adjective; it has real meaning. Some things should not be borne, and that’s bad enough, but some things really cannot be borne. What then? Do we turn our backs and shrug, feeling we’ve done our jobs?
Those who’ve survived the suicide of someone you loved, you have my absolutely heartfelt sympathy. It’s awful, peculiarly and specially awful. There’s nothing like it.
If you’re really outraged, turn your anger onto a suitable target: the systemic failure that made that cherished person’s life unlivable.
That would honor them, in a remarkably constructive way.
I’m off to make sure I’m registered to vote tomorrow. I don’t want to sit this one out. I’m torn up and miserable, and I want to honor the memory of A and all my dear departed angels.
I have loads of advice for surgery and invasive procedures, so I might as well park it in one place. I used to be an RN and I’ve had this monster for over 15 years so I’ll share the key things I know, and others can add more about what they’ve tried or heard about 🙂
NUTRITION
One leg of my Holy Trinity of Healing: Nutrition, Activity, Rest.
ANTIOXIDANTS
With nerve or mitochondrial diseases, antioxidant support is absolutely critical and vitamin C is the cheapest, most bio-available antioxidant. It’s very straightforward — it basically works by refreshing and rebooting the others. The vitamin C protocols for surgeries and procedures with CRPS are simple:
500 MG per dose (more than that, and especially a fragile system will get overwhelmed and throw the whole lot away)
2 to 3 doses per day (2 doses for upper limbs, 3 doses for trunk and lower limbs)
Start up to 2 weeks before surgery
Continue for 3 months (12 weeks) after surgery
Have you had your D3 levels checked? If you’re chronically ill, do so. It’s becoming clear (finally) how crucial this is and how much of it our bodies need in chronic conditions.
D3 is critical for healing, especially joint and bone healing, as well as helping our calcium stay in bones and teeth, helping our skin, and maintaining soft tissue integrity. Get that checked when you can, but if you aren’t already taking it, get started. Something is better than nothing. Raise your dose until your serum vitamin D3 is well within normal range. This is important. The test is relatively cheap and easy to get.
FURTHER NUTRITION
Speaking from decades of clinical and personal experience, I’d add that this is the time to invest in a good, food-based multivitamin and take it with breakfast and lunch every day from now to at least 3 months after your procedure. After years of home care and being a patient myself, I have found nothing — absolutely nothing! — that speeds healing and reduces complications like really good vitamins. It’s like magic. Also, some science is beginning to emerge about the value of nutrition in handling CRPS.
I get my vitamins from vitacost.com, which has wholesale prices and lightning fast shipping, or luckyvitamin.com which has one week delivery. Amazon can sometimes meet those prices, and of course they make it very easy to give them your money.
The brands I can recommend are the capsule (not tablet) forms of:
RAW Vitamin Code (what I use), a Garden of Life line
Irwin Naturals
Garden of Life “My Kind” may be good; it’s new and I haven’t tried it, but its sister line is great.
NOW is normally ok, but it’s not something I’d recommend around a procedure. They’re great for the price, but not top tier. Their multis are tablets which are noticeably harder for fussy systems to handle.
For targeted supplements (Calcium, 5-HTP, DL phenylalanine, magnesium chelates, etc.) I use and recommend (as of 5/2017) these brands:
Jarrow
Pure Formulas
Doctor’s Best
Ester-C
Several other food-based vitamins used to be great but they got bought and really dropped in quality as the parent company squeezed their profits.
Several very famous brands, which I’m not lawyered-up enough to mention, are an absolute waste of money — go to the library and check out the issue of Consumer Reports where they investigated those.
Basically… don’t buy anything you can get in a major pharmacy. When it comes to meds, I always suggest discussing meds with your pharmacist, but when it comes to vitamins, the brands available to them are frauds with great advertising budgets, and they aren’t allowed to say so even if they know it.
Talk this over with a chronically ill person who is a vitamin geek, if you want more recommendations. Some health food stores have good vitamin geeks on staff. Ask around.
RECOVERY
This is based on the 12-week period that covers most procedures and most traumatic injury-healing. This is not for everyone, it’s not comprehensive, it’s just a generic brain-dump from one former RN and current chronic patient. If you’re planning to use this as a guideline, PLEASE take this into your doctor and highlight the bits that matter to you, so you can get a sanity check from the person who’s actually aware of your particular case and is guiding your care.
If your doctor expects less than 12 weeks, smile politely, bless their optimism, and plan for 12 weeks of intensive self-care as the better part of wisdom.
If your doctor expects more than 12 weeks, BELIEVE YOUR DOCTOR. If they tell you to stay in bed for a year, then the survival path and the wise thing to do is to stay in bed for a year. They simply don’t want you horizontal for any longer than strictly necessary, so take them seriously and don’t finesse it. Just don’t even go there. They’ll get you up the very minute it’s even vaguely safe.
Since spoonies are more likely than normal people to have a longer healing period, plan accordingly and mentally prepare a Plan B that includes yet another 25-50% of rehabilitation and recovery time. For each day in bed, figure it will take 1-3 days of activity to recover afterwards, depending on your basic fitness and cardiovascular tone.
It’s okay, don’t let the numbers scare you. I just button on my pig-headedness so it faces the right way, and make myself do the long, slow slog of building back up again. It’s hard work, but the time will pass anyway, and I want to be better at the end of it.
You are not a normal patient, if you already have something like CRPS. Don’t panic; there are lots of abnormal patients out there! You’re not alone. Just plan wisely.
EARLY RECOVERY PERIOD
Early recovery is a bear, but it doesn’t last long. Some things we just have to white-knuckle our way through, one breath at a time. Early recovery may be one of them. It will pass.
At this point, a certain amount of swelling is good and helpful, because it keeps the area flushed with nourishment and growth cells.
Keep your affected body part ABOVE HEART LEVEL if at all possible, to allow the “used” fluid to drain out. Your heart should be able to push the blood up that slope (dysautonomiacs and those with existing circulatory issues, watch this closely), but your body needs a gravity-assist to help it come back down. It also helps keep the pain down. Letting a healing limb hang below heart level will usually immediately increase your pain.
This is where you corral all the pillows you can get your hands on so that, during recovery, you can park that puppy up there and put your head down to lower the bar even further.
Work out a pain management policy in advance with your doctor, so you have a Plan A, B, and C for managing different levels of pain after surgery.
If you’ve had to go to the ER for pain crises before, then ask your doctor to contact the ER and arrange a patient-specific set of interventions for you in case you have an after-hours crisis after surgery. This should ideally:
Be time-limited to the post-surgical period,
Cover both pain and infection and whatever other surgery-specific complications are most likely, and
Indicate when/whether they should call your doctor/surgeon.)
This will save a whole lot of time and fuss, and would make me feel a lot safer about the post surgical period.
Not all ERs make it easy to do that, but you’d be amazed how much silliness a bit of surgeon’s bluster can cut through. The ER will find a way to capture and recall that information all right. They just need a little push sometimes.
Speaking as an old ER nurse, I felt a lot better about treating a chronic patient in crisis according to their specialist’s or surgeon’s requirements, than us having to figure out something so fraught on our own.
Pain crisis and post-surgical emergency protocols tailored to the chronically ill patient are a huge benefit to everyone involved.
There should also be a limit on how many ER visits before your surgeon gets called in, because if you need more than one (maybe 2 on the weekend) then you really need to be seen again by the surgeon on an emergency basis, since something may be wrong with the surgery.
Bones and joints
Those of you with bone and joint trauma or surgery, please be aware that the number 1 cause of non-healing bones is… using the darn things! Here’s the lowdown on fracture (and ligament) recovery:
For the first ~3-5 days, the “callus” is forming. This is the foundation of all the healing that happens after. There is no substitute. This is when there is the most swelling, and there needs to be: there isn’t much blood flow inside bones or connective tissue, so this is the best substitute. Extra hydration (to keep things moving through my tissues) and basic nourishment, featuring vitamins, antioxidants, and digestible protein, is my appropriate dietary focus.
For the next couple weeks, “knitting” is happening. The fractured ends are reaching across the nourished gap and, strand by strand, are pulling together. There’s no hurrying this process, but it’s easy enough to disrupt it, so keep staying off it. Supplementation with bio-available calcium (food-based sources are usually the easiest for the body to get hold of and integrate) with vitamin D, magnesium, and (according to some studies) boron and strontium, can be a real help with rebuilding the bone. I take phosphorus in the middle of the day, because it should not be released into my gut at the same time as calcium, because it’ll block it from being taken in. I take calcium, D, and the other bone-building supplements morning and night.
For the rest of the healing time, the bone break is turning that knitted lattice into solid bone which you will eventually be able to use normally again. I keep up the vitamin and mineral supplementation above, and, trust me, I did absolutely whatever it took to STAY OFF THAT FRACTURE until the bone had gone through its full healing cycle.
After that, it’s just rehab. That takes patience, pacing, and diligence, plus more pain that before, but normally, with the antioxidants and hydration and pacing, it does pass and the bone and muscle are all right at the end of it.
Ligaments take time. They don’t naturally have much blood supply, so they don’t heal quickly. However, with time, nutrition, diligence, and with moving enough to provide as much blood flow to surrounding tissues as your condition permits, these will normally come back in time too. Remember to go easy on that joint’s over-flexion and strain for a couple of years, because it won’t have the old elastic strength for some time.
Organ surgery and trauma
Abdominal surgery usually requires a coughing pillow, to protect healing and allow you to cough and clear your lungs without hurting yourself. (See the part on scar management.) The nurses should set you up with one, but any small, very firm pillow — or a bathtowel folded and taped into shape — will do the job.
Post surgical care for abdominal surgery boils down to:
Keeping your lungs working well. If you can’t breathe well, then you can’t do well. Simple as that.
Keeping your drains — natural and surgical — as clear as possible. (Tips: farts are good! Poop is great! Urine is the key to life!)
Keep moving in small, frequent bursts, so you heal faster — and to help with the previous bullet point.
And, for us painiacs, we add:
Managing pain, so the other stuff (breathing, excreting, moving) is more manageable in turn, and we don’t come out of it worse than when we went in.
You will be discharged with specific instructions about food, fluid, medications, antibiotics, wound care, and so on. FOLLOW THEM.
I know — antibiotics suck and it takes weeks of probiotics and soluble fiber and maybe Senakot to get our guts back in shape. However, the pathogens that can grow in there are far, far worse; finish your antibiotics and kill them dead.Then take the time to rebuild your gut.
I’d love to be able to say otherwise, but that’s the way it is these days; we as a society have to stop creating resistant organisms, and that starts with the ones we, as patients, treat in ourselves.
FIRST 6 WEEKS
The first 6 weeks is the “knitting” part, or, in joint replacement, the part where the bones bind onto the joint insert and make it part of your body.
Keep a close eye on your surgical area for signs of infection or rejection. Be sure your surgeon discusses this in advance so you’re prepared to take the right meds (might be as simple as Benadryl and Advil) at THE FIRST sign of trouble.
For these 6 weeks, the bone care and the skin/nerve care diverge.
Bones
With bone fractures or bone surgeries, NO STRAINING OR BEARING WEIGHT on that part. Do your prescribed physiotherapy if you have any, but don’t go *one ounce* over the line. Pushing it now is the surest way to screw up your healing and have a much bigger and longer-lasting problem.
Just stay completely off the darn thing, ok? Doesn’t matter what it takes.
I’m speaking as someone who crawled to the bathroom on 3 CRPSy limbs (think walking on hands and knees over live coals with hot electric wires sticking out of them, no kidding), 5-6 times a day, for this entire length of time, due to a broken foot. It sucked, but I did it. It was a nightmare and I’d rather shoot myself in the head than go through it again, but I did it, because that’s what it takes to get the bone to knit.
STAY OFF IT. Seriously. Just STAY OFF IT. Figure out how to make that happen, for 6 (in some cases, 8) whole weeks. The time will pass whatever you do, but you’d rather have one less major problem at the end of it, right?
Soft Tissue and Scarring
I scar quickly. This used to be a good thing.
Most scar tissue is laid down in the first 12 weeks, and 50% of that is laid down in the first … I forget.. 2 weeks, or 4? Like I said, my healing rate is odd, so I’m not sure what the usual numbers are.
The first stage of scarring needs to happen as undisturbed as possible, so your tissues can be closed up and the integrity of skin and organs and so forth can be maintained. However, after the first stage (which is when the surgical splints come off), it’s time to start managing the scarring, so that the tissue comes back as close to normal as possible.
Scar tissue is more brittle than regular tissue, especially if left to its own devices. If scar tissue is managed correctly, 3 things will happen:
There will be minimal brittle scar tissue, with minimal risk of subsequent tearing and re-injury.
Regular tissue will grow in and restore normal function, circulation, and flexibility, leaving only a little brittle scar tissue.
Underlying structures, like nerves,vessels, and ligaments, will not be trapped in the scar tissue, so they can continue to function normally.
If scar tissue gets out of hand, those good things don’t happen. And then you have more problems: tearing and re-injury, stiffness and limitations, reduced function in that body part, or, as in my case, nerves and other structures getting completely tied up and trapped in scar tissue (in record time.) Any of these is a whole new set of problems with added complications waiting to pile on.
Some Occupational and Physical Therapists specialize in scar management. Stretching, gentle massage, deeper massage after a certain length of time, silicon pads, heat therapy, bead therapy — they have tons of good tricks up their sleeves.
Case study: Me
I had come out of the post-surgical splint with 4 degrees of motion in my wrist. (That’s not a typo. Check that on a protractor.) Because I was still in the acute-healing phase, the scar tissue was being laid down faster than we could manage it, and if we didn’t have substantial improvement by Week 8 after surgery, I was looking at painful splints and possibly more surgery to loosen up my wrist/forearm so I could use it again.
A warm pack and pain meds, followed in half an hour by diligent massage and stretching for 10 to 20 minutes, three to five times a day, with a silicone pad on it otherwise, was my routine for over a month. I watched a lot of movies to distract from the horrible pain and keep going, because I couldn’t take narcotics — they had hospitalized me with life-threatening side effects.
That’s probably what sealed my fate with CRPS: ineffective and even toxic post-surgical pain control followed by months of brutal rehab with continuing ineffective pain control. We didn’t have a Vitamin C Protocol for hand surgery then, so I didn’t know to take additional antioxidants, the one thing shown to reduce post-surgical CRPS.
Sure wish I’d known that then! It’s so simple, so cheap, so effective!
My wrist has never totally regained all its flexibility, but it used to be freakishly flexible, so it’s technically all right now.
The caution and care you take in these first six weeks will pay off HUGELY. Put your natural stubbornness and self-sufficiency (which most spoonies have a LOT of) in the service of your healing for a month and a half, ok? 🙂
SECOND 6 WEEKS
Now, if things have callused well and knitted properly, the second half of the “12-week healing circus” gets more interesting. This is when you gently and persistently put that part of your body back in service, and remind the nerves there that their job is not to be hysterical and overly dramatic, but to report only/exactly what’s really there. Seriously. It’s a bit like self hypnosis. One great technique is in the “Mental Rehearsal” heading.
Another is a dry version of the Epsom baths described here. Keep in mind that you can use a washcloth or soft cloth dunked in Epsom solution instead of taking a bath, in order to benefit from the de-programming and re-programming you can do on your body in this way.
This period is crucial because that’s when 80-90% of the healing is completed. So, this is why the vitamin protocols, physiotherapy, and medical care really focus on that period. Problems are best found early in this period, so they can be fixed, mitigated, or worked around.
It’s not short, but it is finite!
PHYSIOTHERAPY AND REHABILITATION
Do what you can to get the best rehab possible, and be as communicative and involved as you can. Remember, whether you like your rehab professionals personally is not the point; it’s simply a question of whether you can communicate with them and get the care that you need. If you can’t communicate with them despite your best efforts, change therapists. There has to be 2-way feedback — especially with the tricky cases that we always are — or else it’s not a therapeutic situation.
Retrain the Pain
There are several ways to manage how the CRPS brain mis-handles the new pain information. These are different ways of hacking into the ways that the disease grabs the part of your brain that corresponds to the part of your body that CRPS wants to climb into.
Naturally, there are no guarantees, but mental-plasticity techniques can be hugely helpful.
Mental Rehearsal
When you are using that limb in the rehab stage, mentally practice the motion first, playing it out painlessly in your mind. Imagine the whole motion going perfectly comfortably. Then do the motion. If this doesn’t go well, work with your physical therapist on details of the technique (there are several ways to conduct the imaginary and real movements) and figure out what works best for you. Persistence is key in rehab.
The point is to make the movement you mentally practice as realistic as possible, as much like the real motion as possible, and have it be painless and comfortable in your mind when you practice it. Keep doing the mental rehearsal before the movement, and refine the mental rehearsal until you can predict the shape of your movements fairly exactly. This was one of the best tricks I ever learned for de-programming my body’s pain responses and getting back a TON of function.
If done wrong, it can have pretty much the opposite effect, so go carefully and find good guidance if it’s not easy for you.
Brushing
This is kind of like acting out a metaphor, and that metaphor communicates with the body-mapping parts of the brain in a way it’s hard for them to ignore.
I find it makes a big difference if I approach all this with an attitude of parental authority toward my own body. I can’t control my body completely, just as a parent can’t completely control a child, who really is a separate entity; but a parent can exert a great deal of influence, when they do so with tones of loving, generous, insistent declaration.
“This is best for you, and I know that, and what happens to you matters, so do this and we’ll go from there.”
For paraesthesias — the garbage-can term meaning “weird skin sensations”, including numbness, tingling, or allodynia — I simply stroke from a non-weird area into the weird area.
I pay attention while I’m doing that, mentally pushing the non-weirdness into the weird area, and telling the weird area to pay attention because this is what “normal” feels like and “normal” is the appropriate way to feel. Kindly persistence is key.
Every now and then, I hear Jim Carrey’s character talking to his dog Milo. This clip isn’t in English, but somehow the meaning comes through in the first minute: “Come here, Milo… Come on, there’s a good boy… You can do it… PUT SOME EFFORT INTO IT!”
PAIN REHABILITATION can take longer than 12 weeks! Keep at it
Be patient. Be diligent. Above all, don’t give up. It just takes time (months or years in some cases) but it can usually be done, and the time will pass either way so you might as well have something to show for it.
Keep working on it. Mental rehearsal, brushing, self-hypnosis, calming meditation, Epsom baths, vitamins, etc. It all helps. Keep at it.
If you don’t already have a good pain psychologist, this is the time to get that referral. Pain psychologists have special training around understanding how pain impacts the brain, and how this, in turn, affects our feelings and behavior, and what we can do about that. Most importantly, they have special training about how to use the characteristics of the brain to better our frames of mind under varying stresses. It’s pretty brilliant.
There is a ton of good science on how we can learn to use our minds to improve our lives, and pain psychologists are the ones trained in how to identify our strengths and struggles and train us as individuals in using the tools that can benefit us the best.
NUTS-AND-BOLTS PREPARATION FOR PROCEDURES AND SURGERIES
Basic activities of life have to go on… So, plan ahead, clear the decks for action, and prepare some things ahead of time so that you have less to flail about when the time comes.
FOOD
You need to be able to get a meal with minimum effort for a couple of weeks. Before surgery, stock up on easy food. For me at my surgeries, that was apples and nut butter, nitrate-free cold cuts and veggie chips, romaine lettuce and Cabot Extra Sharp cheddar — which I slice and bag up ahead of time. Trader Joe’s and good grocery stores often have pre-made wraps, soups & salads, and good frozen meals. For normal people with fewer allergies, it’s probably instant soups and microwaveable food. Whatever works for you. As long as you’re taking your vitamins, packaged food may be a reasonable compromise within your limits.
Say it with me: “Do what works for you.”
Clean clothes and sheets
Also, catch up on laundry and get rid of any “stupid problems” around the house — a door that makes you fight with it, a sink stopper that doesn’t work, a rug that always catches your foot. Fix the door, pull out the broken stopper and replace it with one from the dollar store, and get rid of the rug. I hate those kinds of rugs. (Old trauma nurse, remember.)
Making a “day nest”
If you don’t already have one, set up a “day nest” at home. It’s absolutely essential to get out of bed every day if possible, because it’s much better for your brain, but for awhile you won’t be up to much more. Make a comfortable place to lounge and watch tv, with your body-part up, some kind of toileting you can get to, and your comfort kit handy (books, comics, hot water bottle, meds, snacks, etc.) for hours at a time.
Personal hygeine (sigh)
You’ll need to waterproof that body part for bathing and showering. You may need back scrubbers and other reaching aids to get clean, too. At certain times, a wet washcloth may be the best you can do, so make it easy to reach the washcloth, soap, and a manageable towel.
Try to work this out ahead of time. Give yourself slack for different levels of ability: washcloth while sitting on the toilet, soaking in the bath with the body part perched on the rim, showering in a chair or stool, or standing under the running water. Remember to figure out how to clean and manage your hair.
Having this mapped out ahead of time simplifies the hygeine. For another, it’s powerfully healing to know that you’re taking good care of yourself.
The first few days are… special
I find that the first 2-3 days are too bewildering and painful to handle alone. After that, I’d begun to learn how to change position, dress, and wipe myself adequately (hey, that’s important!) and the IV site had healed.
If you’re on your own normally, try to find a helpful friend to stay with (or ask them to stay with you) for the first 2-3 days. All you need is someone to remind you that there’s life outside this, to pass your meds and a tissue, and, if necessary, call an ambulance to get you to the ER. Simple enough.
Final Notes
If you’re facing surgery or invasive procedures or a major injury, you’ve got a tough gig ahead of you, but you can manage it. I’d be wetting myself with anxiety if I had to face that again, but I’d do all this stuff anyway because I know it works.
Now, having said that, this is the part where I have to insert the reminder that I am not a doctor, I have not examined my readers, and I have no business making diagnoses or conducting treatments on them.
Since I’m a pretty straightforward old cuss, I’ll add that it’s your own body anyway and you have to do your own homework, follow your own inner promptings, and take responsibility for the choices you make accordingly.
May all things go well for you, especially recovery.